








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


Bone Transplantation with Systemized Armamentarium
Streckbein, Roland -

Regenerative Treatment of Class II Mandibular Furcation Defects
Heinz, BerndProcedure Case description: -Class II furcation defect at teeth 46 and 47 and gingival recessions at teeth 43 and 44 - Root planing using PerioSet - Incision technique - Cleaning furcation defect at tooth 46 - Pref Gel application, rinsing and Emdogain application - Insertion of Bio-Oss into the furcation space with an amalgam plugger after hydration - Condensation of the bone replacement material and application of an absorbable membrane (Bio-Gide) - Atraumatic suture closure using 6/0 Seralene Contents: This video demonstration shows the simultaneous treatment of recessions at teeth 43 and 44 and of class II furcation defects at teeth 46 and 47. After a brief case description, root planning is done using PerioSet. Next, an incision is made and the furcation defects are very carefully cleaned using hand instruments and ultrasonic scalers (Soniflex). The cleaned root surfaces and furcation defects are conditioned with Pref Gel (Straumann) for two minutes. The objective of conditioning is to remove the smear layer, to open the dentine tubules, and to enable surface demineralization. Moreover, this measure serves to optimize the contact between Emdogain and the root surface. After two minutes, the EDTA suspension is removed using physiological saline solution or water spray. Immediately afterwards, Emdogain is applied to the blood and saliva-free root surface. This procedure was also used to treat the furcation defect at tooth 47. Regenerative treatment of tooth 46 was performed since that tooth had a very extensive furcation defect. The defect was filled with Bio-Oss, which was applied using an amalgam plugger. Absorbable Bio-Gide was used for coverage of the furcation entrance. Finally, the wound was closed using loop sutures and single interrupted sutures. -

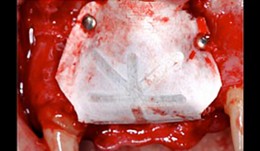
Regenerative Procedures for Optimized Esthetics at Tooth 11
Schlee, MarkusContents: - Exploration - Incision and Flap Mobilization - Palatal Flap Preservation with Interdental Tissue Preservation - Detoxification and Concrement Removal at 11 - Harvesting of Autogenous Bone Chips from the Spina Nasalis - Conditioning of the Root Surface with EDTA-Gel - Application of Emdogain and Filling of the Bone Defect - Wound Closure Synopsis After Finishing the Initial Treatment for Aggressive Periodontitis, Regenerative Treatment of a Tunnel-Shaped Pocket at Tooth 11 was attempted. Rotation and Crowding of the Buccally Inclined Tooth represented a favorable Etiological Factor. The patient did not wish to receive Orthodontic Treatment to eliminate this Causal Factor after Completion of Primary Treatment. Treatment was therefore limited to the Surgical Regeneration Attempt. The Interdental Space was larger than 3 mm and the Bone Pocket was a mostly Three-Walled Structure, so the Chances of Success were considered to be good. Exploration was first performed to identify the Course of the Defect Margins. Exact knowledge of the Bone Anatomy in all three Planes is essential to successful Incision Planning. A Tunnel-Shaped Defect delimited by Bone in the Region of Tooth 11 with good chances of Periodontal Regeneration was found. A major Challenge of this Procedure is the need to keep the Defect completely covered with Soft Tissue throughout the Healing Process. Cortellini's Papilla Preservation Technique was used for this Purpose. After Incision and Flap Mobilization, it became evident that the Defect only had two Walls in the Coronal Region and that Bone was lacking in the Buccal Region. According to the current Data on Periodontal Regeneration, the Attachment Gain achieved using an Enamel Matrix Protein (Emdogain®) alone can be just as good as that achieved using Emdogain and Bone Graft Material combined. Still, we elected to use a Combination Technique in the Present Case because it provides better Papillary Support. The Graft Material consisted of Autogenous Bone Chips from the Spina Nasalis, which can easily be harvested by Means of the Piezo Technique After gentle Detoxification, the Root Surface was treated with Emdogain. The Defect was then filled with Autogenous Bone Chips and closed by Microsurgical Suture Techniques. Six months after Surgery, Partial Regeneration of the Papilla can be seen. -

Combined implant treatment with soft and hard tissue management
Schlee, MarkusProcedure - Soft and hard tissue management - Implantodontic treatment - Case documentation Contents: - History - Patient hadn't seen a dentist for 15 years - Has been on Marcumar since developing a blood clot in 1997 - His general practitioner extracted teeth and performed conservative dentistry during the last year - Heavy smoker (30 cigarettes a day) - Prothrombin time (Quick's value): 40 - Premedication: Augmentan 750/125 tablets. -

Bone Transfer
Streckbein, RolandContent: Description of system and instruments. The patient had a considerable bone deficit at tooth 21. Augmentation was therefore required and was carried out using calibrated instruments. The augmentation site was prepared using instruments that matched the tools used to harvest the cylindrical bone graft at the donor site. This perfect match between the augmentation region and the bone transplant accelerated osseointegration, there by shortening the required waiting time for implant placement. -

Sinus Bone Augmentation with PRP
Schultze-Mosgau, StefanContents - Incision technique for lateral sinus floor augmentation - Creation of a lateral bone window in the facial maxillary sinus wall - Maxillary sinus floor elevation - Chin bone graft harvesting - Retromolar bone harvesting - Sinus floor augmentation using autologous bone, beta- tricalcium phosphate (1:1) and PRP Synopsis: Maxillary sinus augmentation may be indicated in cases where it is desirable to increase the vertical bone stock in the upper lateral tooth region. Maxillary sinus floor augmentation entails the implantation of autologous bone or bone replacement material in the spaces between the bony floor and elevated membrane of the maxillary sinus. This video demonstrates the techniques for palatal incision, access preparation, and exposure of the facial wall of the maxillary sinus. A diamond drill is used to create a bony window in the facial wall of the maxillary sinus taking care not to perforate the sinus membrane. After completely detaching the basal parts of the membrane, the flap is advanced cranially using angular elevation instruments. Regarding the procedure for autologous bone grafting, the steps for incision, prepping and harvesting of monocortical chin bone transplants with a trephine drill are demonstrated. An alternative procedure for harvesting retromolar bone material is also shown. A bone mill is used to particulate the autologous bone material. The autologous bone chips are then mixed 1:1 with beta-tricalcium phosphate (and PRP) and inserted in the sinus floor. -
Minor bone regeneration procedures
Prof. Christer DahlinIn this module Prof. Christer Dahlin explains the principles of minor bone regeneration procedures. The focus is on the biologic principles of GBR, the importance and the choice of membranes, the characteristics of different bone substitute materials and the potential future developments. -

Alveolar ridge preservation
PD Dr. Ronald JungWhen a tooth is considered to be irrational to treat and needs to be extracted every dentist needs to take decisions on whether to let the socket heal spontaneously with a blood clot or whether to perform alveolar ridge preservation procedures. In this module you are going to learn all the important decision-making factors and the clinical handling after tooth extraction to chose either between spontaneous healing after tooth extraction or immediate implant placement or alveolar ridge preservation procedures. -

Implant timing
PD Dr. Ronald JungIn every clinical situation, which is scheduled for an implant placement, a decision needs to be taken in regards to the right time after tooth extraction to insert the implant. In this module you are going to learn all the important decision-making factors (anatomical, esthetical, clinical, radiographical and patient centered) to chose the correct timing for implant placement after tooth extraction. -

Esthetic and functional restoration
Thomas HitzThe old restorations showed several ceramic fractures and in some areas the framework was exposed. The patient's main concern was the unesthetic appearance of the anterior crowns in the maxilla due to these chippings. -

Esthetic and functional rehabilitation
Sven Mühlemann58-year-old woman desires a total refurbishment by reason of compromised esthetics of her front teeth and missing teeth in the upper left jaw. In addition the bridges in the mandibular left and right show chippings. -

Esthetic and functional dental rehabilitation
Dr. Dominik BüchiMale patient (*1955) treated by Dr. D. Büchi. Functional and esthetic rehabilitation through replacement of insufficient crowns and bridges. Additionally implants were placed in the posterior part, to maximize the masticatory performance.