








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


Bone Transplantation with Systemized Armamentarium
Streckbein, Roland -
ACHIEVING A MORE EFFICIENT CONTACT SURFACE BETWEEN A BLOCK BONE AND RECIPIENT AREA USING A 3D STEREOLITHOGRAPHY (SLA) MODEL OF A JAW FRAGMENT IN ADJUSTING A HUMAN BONE BLOCK TO THE RESIPIENT AREA AND TIME SAVING DURING OPERATION
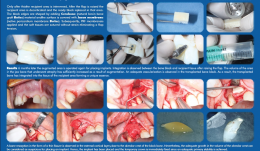
Objectives: Autogenic and allogenic bone block materials of different companies are increasingly used in guided bone regeneration (GBR) procedures. Adjusting block-shaped allogenic transplants to fit the recipient area is time consuming and technically challenging. A method of bone block formation using a 3-D stereolithography (SLA) model is reported here. Methods: A tomographic image of the area for augmentation was obtained and edited using Implant Assistant. Data from the image of the prepared 3-D jaw model were transferred to a 3-D printer (Objet Stratasys to produce a model of the jaw fragment. Unicortical cancellous block (Maxgrapht cortico-spongiosa) was moulded onto the model and holes for fixation screws were drilled into the material. The bone block was added to a 100-grams syringe filled with serum, emptied out in to a container and refilled. This procedure was repeated several times. After raising a flap, the recipient area was decorticated and the prepared block put in place. The edges were shaped by adding natural bovine bone graft (Cerobone) material and the surface was covered with native pericardium membrane (Jason membrane). A platelet-rich fibrin (PRF) membrane was then applied and the soft tissues sutured without strain to avoid flap tension. Results: After 6 months, the augmented area was re-operated for implant placement. Integration was observed between the bone block and recipient tissue after raising the flap. The volume of jaw atrophied bone had increased as a result of augmentation. There was adequate vascularisation of the transplanted bone block, which was integrated into the tissue of the recipient area. Bone resorption in the form of a thin fissure was observed in the external cortical layer, close to the alveolar crest of the block. Nevertheless, the growth in alveolar crest volume was deemed adequate for implant placement. A temporary crown was fixed immediately after placement because there was adequate stability, and alveolar crest defect was re-grafted with Cerabone and covered with Jason membrane before the flap was closed. After 4 months, an image was taken that showed bone augmentation and osseointegration around the implant. Conclusions: Preparing a jaw bone fragment as an allogenic bone block using an SLA model done successfully in GBR-type surgeries. The method allows block bone to be adapted for the recipient area, and is associated with significant time savings. Post-operative tomographic scans confirm augmentation of the alveolar ridge, making this a promising way for restoring aesthetics in the frontal area. -

STEM CELL BONE ALLOGRAFTS IN MAXILLARY SINUS AND RIDGE AUGMENTATION – REPORT OF A CASE
Objectives: To evaluate the use of an allograft cellular matrix containing live stem cells for maxillary sinus and ridge augmentations. Methods: Maxillary sinus and ridge augmentations were performed using an allograft cellular matrix containing live stem cells. The post-operative results were evaluated by CT scans and peri-apical radiographs. Sinus augmentation was evaluated after 10 weeks. Radiographic bone tomography was similar to that of the native bone and the ridge augmentation resulted in a vertical ridge augmentation of 3–4mm. The cellular matrix was supplied by Brockton, MA and processed by AlloSource, Centennial, CO. Results: Following healing and approximately 10 weeks following surgery, an additional CT scan was taken. This showed that the native and augmented bone was of an adequate width for supporting an implant. Radiography revealed that the augmented bone had a similar texture to native bone, indicating formation of mature bone. The scan also revealed downward growth of the bone in a vertical direction, overlapping the crest of the native pre-maxillary bone. This was not attempted during the surgical procedure, and was a particular cause for concern. Conclusions: This use of allograft mesenchymal stem cells has been shown to be a reliable method for ridge augmentation, especially in the vertical direction in areas of severe ridge atrophy. Further studies are needed to support this finding in a more guided manner, especially for vertical ridge augmentation. -

-

-

-

-

-

-

-

-
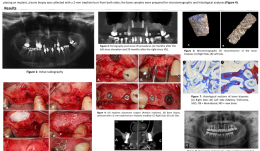
BONE FORMATION AT 12 MONTHS AND 20 MONTHS AFTER SINUS ELEVATION SURGERY WITH INORGANIC BOVINE BONE—A SPLIT-MOUTH CASE REPORT WITH MICROTOMOGRAPHIC AND HISTOLOGICAL EVALUATION
Objectives: Rehabilitation of the posterior edentulous maxilla using a dental implant is challenging when bone volume is limited. The literature supports the use of sinus lift procedures for increasing bone volume by filling the sinus cavity with autogenous bone and/or bone graft substitutes. This study reports on a patient with clinical, tomographic, microtomographic and histomorphometric evaluation of the resorption of Bio-Oss[tm] after maxillary sinus floor augmentation. Methods: A 55-year-old, non-smoking woman presented with limited bone volume on both sides of the posterior edentulous maxilla that required rehabilitation. She had no systemic problems that might affect the surgical procedures. Preoperative cone-beam CT revealed significant maxillary sinus pneumatisation. Sinus lift procedures were performed on both sides of the maxilla, using a lateral surgical approach, and the maxillary sinuses were filled with a bovine bone graft substitute (BioOss[tm] small particles). A 25x25-mm collagen membrane (BioGide[TM]) was placed over the graft and the surgical flaps were sutured to entirely cover the membranes. Postoperative medications were amoxicyillin 500mg, clavulanic acid 125mg, ibuprofen 200mg and PerioGard[TM] rinse. Sutures were removed 14 days after surgery. Healing was uneventful, with no membrane exposure or other complications. After 12 months, further cone-beam CT showed significant gains in bone volume in both maxillary sinus areas, supporting the installation of osseointegrated implants. The patient postponed implant placement surgery; the left side was reopened 12 months after sinus lifting and the right side after 20 months. Before placing an implant, a bone biopsy was collected with a 2-mm trephine bur from both sides and samples were prepared for microtomographic and histological analysis. Results: Four months after implant installation, the healing abutments were connected and cone-beam CT was performed to evaluate the implants. Provisional prostheses were then installed and remained in function for 3 months, allowing functional analysis of the prosthetic rehabilitation. Definitive ceramic crowns were then installed. Microtomography showed newly formed bone (27%) and residual biomaterial (39%). Biopsy samples at 20 months post-operatively contained [ok?] 52% newly formed bone and 16% residual biomaterial. These results revealed the process of particle resorption and replacement by new bone tissue between 12 and 20 months. Histological analysis demonstrated remnants of biomaterial particles surrounded by newly formed bone without connective tissue. There were no signs of inflammation and there was no gap between the bone and Bio-Oss[tm] particles. The biopsy collected at 20 months showed noticeably fewer particles of residual biomaterial than that collected at 12 months. Conclusion: This report showed that an inorganic bovine bone graft associated with collagen membrane can be used successfully in this sinus lift procedure for the subsequent installation of dental implants. There was slow resorption of particles and continuous replacement by newly formed bone, which are desirable for to maintaining grafted bone volume for a longer period. It is important to emphasize that this report is not intended to change the protocol for installation of implants after sinus lifting using inorganic bovine bone and collagen membrane. The extended implant placement times (12 and 20 months) described here related to the patient's situation and are not necessary or desirable in clinical practice.