








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


Study Protocols: Maxillary Sinus Floor Elevation
based on the book chapter by Gustavo Avila-Ortiz andPablo Galindo-Moreno Summary This technique is used to gain bone height in posterior atrophic maxillary segments before implant placement. It is increasingly used in patients with maxillary sinuses that are too close to the upper jaw or excessive bone reabsorption from gum disease. Endpoints relate to the amount of new bone formation after grafting and survival of implants and implant-supported prostheses. and long-term success rates are high. It is also excellent for studying healing following grafting with different materials and regenerative strategies in large craniofacial defects. The protocol described here is based on a hypothetical study, and covers patient screening, selection, enrolment and randomization, including a sample size calculation (which is omitted in most published studies). There are multiple phases for planning and executing the sinus elevation, followed by post-operative evaluation, and further planning and placement of implants. Detail is given on the length and form of patient visits for evaluations using cone-beam CT, impressions, photos, clinical measures, bone biopsies and adverse events recording. The discussion is supplemented by images of bone core histology and diagrams of the paranasal sinuses, and the authors point out the difference between crestal and lateral approaches. The lateral approach is illustrated throughout, including follow-up at 24 weeks and implant placement. The authors also address the problems of membrane perforation and nasal meatus occlusion. Open full-text PDF (1.9 MB) -

Bone Spreading, Bone Condensing (Split Control System)
Streckbein, Roland -
Mandibular Distraction Osteotomy
Schleier, Peter / Schultze-Mosgau, StefanProcedure - Indications and preoperative planning - Incision technique and osteotomy - Placement of distraction apparatus - Wound closure and postoperative regimen Materials: V2-Alveolar distractor, Medartis (Switzerland) 2,0mm Screws for Osteosynthesis, Medartis (Switzerland) Vicryl Suture, Ethilon (USA) -

Sinus Floor Augmentation with Autogenous Chin Bone Grafts
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: In the maxillary incisor region, a sinus floor augmentation to enlarge the vertical bone supply may be indicated for a vertically reduced local bone height of less than 5 to 7 mm before procedures to rehabilitate masticatory function with an implant-bearing tooth replacement. For a single-sided deposit osteoplasty, the quantity of autogenous bone from the chin region is usually sufficient. The operative procedure of a single-sided lateral sinus floor augmentation is demonstrated with particulate spongious bone and alternatively with an autogenous block graft. The video also shows the operative method for a crestal sinus floor augmentation with the aid of the endoscopically controlled condensation technique. The advantages and disadvantages of the individual procedures are highlighted. In addition, the technique for harvesting chin bone transplants in different case examples is shown. Outline: - Operative technique for lateral sinus floor augmentation with autogenous particulate spongious bone - Operative technique for lateral sinus floor augmentation with autogenous block grafts - Crestal, endoscopically controlled sinus floor augmentation with condensation technique - Techniques for harvesting chin bone grafts - Range of indication for sinus floor augmentation - Lateral sinus floor augmentation - Operative technique of crestal, endoscopically controlled sinus floor augmentation - Operative technique of autogenous chin bone removal -

Defect Prevention following Extraction of a Maxillary Central Incisor
Zuhr, OttoContents: - Minimally invasive, atraumatic extraction of an anterior tooth - Buccal soft tissue augmentation using a modified tunneling technique - Socket preservation technique for conservation of the extraction socket - Provisional restoration and closure using modified suspension sutures Materials Checklist: Tunneling Knife® (Dr. Zuhr), No. 1 / No. 2 Keydent Microblade SR Geistlich Bio-Oss® Spongiosa, particle size 0.25 - 1 mm Geistlich Bio-Gide® membrane, 25 x 25 mm Seralene Blue 7/0 DS-15, 0.5 m sutures CV-5 Gore-Tex sutures -

Ridge augmentation in the periodontally involved dentition
Windisch, PéterContents: - Periodontal regeneration and alveolar -ridge augmentation using a connectivetissue graft - Implant insertion and augmentation - Implant re-entry and prosthetics Materials Checklist Emdogain, Bio-Oss, BioGide, Block fixating screw for autologous bone cylinder, 4/0 and 5/0 sutures, Resolut membrane Titanium pins, Autologous bone chips, 2 Replace Groovy Tapered 4, 3x13 mm implants -


-

Implant Bone Dentures with Bone Augmentation and Soft Tissue Transplantation for Papillary Regeneration (Clinic and Laboratory)
Körner, Gerd / Müterthies, KlausDrill guide preparation with the aid of a temporary; Bone augmentation using a bone block graft; Implant insertion; Augmentation of gingival margin with a soft tissue graft from the roof of the mouth; Preparation of tooth replacements according to esthetic criteria, in some cases, as all-ceramic crowns. -

-
Study Protocols: Horizontal Ridge Augmentation
based on the book chapter by Nikos Donos and Nikos Mardas Summary This protocol focuses on measuring radiographic bone levels on the buccal side of augmented areas around implants after horizontal ridge augmentation, rather than at interproximal sites (a limitation of most published studies). The design offers a standardized means to assess graft materials, bone fillers and bone substitutes for horizontal ridge preservation, allowing comparisons of resorbable and non-resorbable materials and natural and synthetic membranes. It includes two randomized controlled trials for patients with bone defects from destructive gum disease who need local ridge augmentation before implantation. One trial uses a simultaneous technique whereby implants are placed in bone augmented with a new bone substitute plus a new or standard membrane, or a standard collagen membrane plus deproteinized bovine bone mineral; this trial comprises two phases surgical implantation and observation. The other trial is a staged technique comprising a new block-bone graft/substitute plus a new or standard membrane, and autogenous block bone graft plus a standard collagen membrane; this has a third phase. A 1-year timeline and 5-year follow-up is suggested for both trials. The authors cite various histologic and radiographic endpoints, photon bubble oscillations, peri-implant bone preservation, implant survival, patient morbidity, adverse events and patient-related outcomes. Images are provided of the change in bucco-palatal/lingual alveolar ridge width 6 months after the procedure. Open full-text PDF (1.3 MB) -
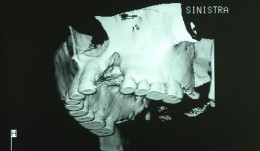
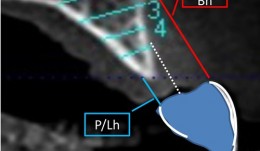
Study Protocols: Vertical Ridge Augmentation
based on the book chapter by Isabella Rocchietta, David Nisandand Massimo Simion Summary This chapter reviews the need for standardized research into vertical ridge augmentation procedures because restoring bone volume after trauma or disease is clinically challenging; the outcomes are unpredictable, the complication rates are high and success is limited. The presented protocol involves initial augmentation surgery comprising a composite graft of autogenous bone and deproteinized bovine bone, with tenting screws and a PTFE membrane overlay, followed 6 months later by surgical removal of the membrane and screws and placement of an implant. Guided bone regeneration is compared with a gold standard two-stage procedure using autogenous bone strips with deproteinized bovine particles and a titanium-reinforced membrane. The timeline incorporates a 6-month evaluation phase and further evaluation 4 months later, with a 5-year follow-up. Patient numbers and selection criteria are defined, along with suitable endpoints, care routines and the use of cone-beam CT to assess bone gain and quality. The descriptions are illustrated by CT images, radiographs and clinical photographs that show preparation of the donor and implant sites in both surgical phases. The evaluation phase relates to responses of the defect over time in terms of resorption of graft particles, soft tissue swelling, inflammation, and bone destruction and formation. What the protocol aims to do is improve outcomes for patients with traumatic tooth extractions, jaw damage, endodontic infections and failed implants. Open full-text PDF (1.4 MB) -

Treatment of a fenestration defect with GBR and CT graft
João Batista Cesar Neto