








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


Immediate Function with NoblePerfect Implants
Nölken, RobertProcedure: - Extraction of upper front teeth not suitable for preservation - Immediate loading of four NobelPerfectTM implants - Intraoperative registration of implant position - Flap-free Vestibular Bone Augmentation - Connective Tissue Graft for Periodontal Regeneration - Immediate Loading of temporary implants on the day of surgery - Definitive restoration 6 months later Materials: NobelPerfect Groovy Implants RP and NP; NobelPerfect Temporary Abutments RP and NP; NobelPerfect Implant Replicas RP and WP; Ribbond, Bondable Reinforcement Ribbon; Ethilon 5-0 FS3 Suture Material; Astra Bonetrap Bone Collector. -

Prosthetic Planning and Prosthetically Guided Minimally Invasive Implantation
Rammelsberg, Peter / Hassel, AlexanderContents: - Considerations for prosthetic treatment planning (PowerPoint) - Production of the drill guide according to prosthetic specifications (PowerPoint) - Surgical procedure (film) - Flapless surgery - Access preparation - Pilot drilling using the drill guide - Preparation of the implant site - Internal sinus lift - Implantation Materials Checklist: Pilot drill; Alignment pin, depth gauge Straight osteotome for bone condensation (Ø 3.5 mm); Larger drills to enlarge the osteotmy; Round burs; Osteotome, angled, for sinus lift (Ø 4.2 mm); Ratchet, adaptor for ratchet (short); Holding key for transmission, SCS screwdriver (short); STRAUMANN Standard Plus RN implant (Ø 4.1 mm, L: 12 mm) and healing abutment (2 mm); STRAUMANN Standard Plus WN implant (Ø 4.8 mm, length 12 mm) and healing abutment (3 mm); Scalpel blade (15c) and scalpel blade holder (Martin); Two dental mirrors and dental forceps; Surgical forceps; Anatomical forceps; Probe; Periodontal probe; Sharp spoon; Sterile compresses (Hu Friedy); Isotonic sodium chloride solution, 0.9% (Braun). -

Preimplant Augmentation Procedures to Improve the Hard Tissue Situation in the Upper Anterior Region
Mayer, MatthiasContents - Flap design according to the layering technique - Piezoelectric bone surgery - Bone spreading with osteotomes - Augmentation and suturing Materials Checklist: Piezo surgery unit (ADS); Osteotome (Altatec GmbH); Surgical tray, individual. -

Regenerative Treatment of Class II Mandibular Furcation Defects
Heinz, BerndProcedure Case description: -Class II furcation defect at teeth 46 and 47 and gingival recessions at teeth 43 and 44 - Root planing using PerioSet - Incision technique - Cleaning furcation defect at tooth 46 - Pref Gel application, rinsing and Emdogain application - Insertion of Bio-Oss into the furcation space with an amalgam plugger after hydration - Condensation of the bone replacement material and application of an absorbable membrane (Bio-Gide) - Atraumatic suture closure using 6/0 Seralene Contents: This video demonstration shows the simultaneous treatment of recessions at teeth 43 and 44 and of class II furcation defects at teeth 46 and 47. After a brief case description, root planning is done using PerioSet. Next, an incision is made and the furcation defects are very carefully cleaned using hand instruments and ultrasonic scalers (Soniflex). The cleaned root surfaces and furcation defects are conditioned with Pref Gel (Straumann) for two minutes. The objective of conditioning is to remove the smear layer, to open the dentine tubules, and to enable surface demineralization. Moreover, this measure serves to optimize the contact between Emdogain and the root surface. After two minutes, the EDTA suspension is removed using physiological saline solution or water spray. Immediately afterwards, Emdogain is applied to the blood and saliva-free root surface. This procedure was also used to treat the furcation defect at tooth 47. Regenerative treatment of tooth 46 was performed since that tooth had a very extensive furcation defect. The defect was filled with Bio-Oss, which was applied using an amalgam plugger. Absorbable Bio-Gide was used for coverage of the furcation entrance. Finally, the wound was closed using loop sutures and single interrupted sutures. -

Bone Transplantation with Systemized Armamentarium
Streckbein, Roland -
ACHIEVING A MORE EFFICIENT CONTACT SURFACE BETWEEN A BLOCK BONE AND RECIPIENT AREA USING A 3D STEREOLITHOGRAPHY (SLA) MODEL OF A JAW FRAGMENT IN ADJUSTING A HUMAN BONE BLOCK TO THE RESIPIENT AREA AND TIME SAVING DURING OPERATION
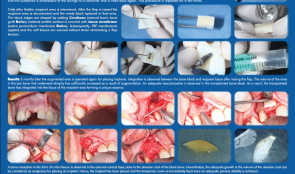
Objectives: Autogenic and allogenic bone block materials of different companies are increasingly used in guided bone regeneration (GBR) procedures. Adjusting block-shaped allogenic transplants to fit the recipient area is time consuming and technically challenging. A method of bone block formation using a 3-D stereolithography (SLA) model is reported here. Methods: A tomographic image of the area for augmentation was obtained and edited using Implant Assistant. Data from the image of the prepared 3-D jaw model were transferred to a 3-D printer (Objet Stratasys to produce a model of the jaw fragment. Unicortical cancellous block (Maxgrapht cortico-spongiosa) was moulded onto the model and holes for fixation screws were drilled into the material. The bone block was added to a 100-grams syringe filled with serum, emptied out in to a container and refilled. This procedure was repeated several times. After raising a flap, the recipient area was decorticated and the prepared block put in place. The edges were shaped by adding natural bovine bone graft (Cerobone) material and the surface was covered with native pericardium membrane (Jason membrane). A platelet-rich fibrin (PRF) membrane was then applied and the soft tissues sutured without strain to avoid flap tension. Results: After 6 months, the augmented area was re-operated for implant placement. Integration was observed between the bone block and recipient tissue after raising the flap. The volume of jaw atrophied bone had increased as a result of augmentation. There was adequate vascularisation of the transplanted bone block, which was integrated into the tissue of the recipient area. Bone resorption in the form of a thin fissure was observed in the external cortical layer, close to the alveolar crest of the block. Nevertheless, the growth in alveolar crest volume was deemed adequate for implant placement. A temporary crown was fixed immediately after placement because there was adequate stability, and alveolar crest defect was re-grafted with Cerabone and covered with Jason membrane before the flap was closed. After 4 months, an image was taken that showed bone augmentation and osseointegration around the implant. Conclusions: Preparing a jaw bone fragment as an allogenic bone block using an SLA model done successfully in GBR-type surgeries. The method allows block bone to be adapted for the recipient area, and is associated with significant time savings. Post-operative tomographic scans confirm augmentation of the alveolar ridge, making this a promising way for restoring aesthetics in the frontal area. -

STEM CELL BONE ALLOGRAFTS IN MAXILLARY SINUS AND RIDGE AUGMENTATION – REPORT OF A CASE
Objectives: To evaluate the use of an allograft cellular matrix containing live stem cells for maxillary sinus and ridge augmentations. Methods: Maxillary sinus and ridge augmentations were performed using an allograft cellular matrix containing live stem cells. The post-operative results were evaluated by CT scans and peri-apical radiographs. Sinus augmentation was evaluated after 10 weeks. Radiographic bone tomography was similar to that of the native bone and the ridge augmentation resulted in a vertical ridge augmentation of 3–4mm. The cellular matrix was supplied by Brockton, MA and processed by AlloSource, Centennial, CO. Results: Following healing and approximately 10 weeks following surgery, an additional CT scan was taken. This showed that the native and augmented bone was of an adequate width for supporting an implant. Radiography revealed that the augmented bone had a similar texture to native bone, indicating formation of mature bone. The scan also revealed downward growth of the bone in a vertical direction, overlapping the crest of the native pre-maxillary bone. This was not attempted during the surgical procedure, and was a particular cause for concern. Conclusions: This use of allograft mesenchymal stem cells has been shown to be a reliable method for ridge augmentation, especially in the vertical direction in areas of severe ridge atrophy. Further studies are needed to support this finding in a more guided manner, especially for vertical ridge augmentation. -

-

-
