








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


-

-

-

-

-
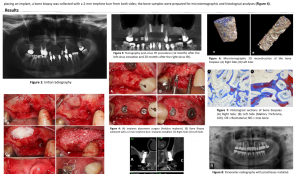
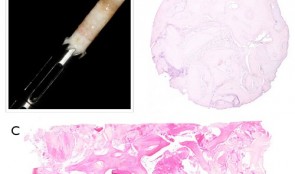
BONE FORMATION AT 12 MONTHS AND 20 MONTHS AFTER SINUS ELEVATION SURGERY WITH INORGANIC BOVINE BONE—A SPLIT-MOUTH CASE REPORT WITH MICROTOMOGRAPHIC AND HISTOLOGICAL EVALUATION
Objectives: Rehabilitation of the posterior edentulous maxilla using a dental implant is challenging when bone volume is limited. The literature supports the use of sinus lift procedures for increasing bone volume by filling the sinus cavity with autogenous bone and/or bone graft substitutes. This study reports on a patient with clinical, tomographic, microtomographic and histomorphometric evaluation of the resorption of Bio-Oss[tm] after maxillary sinus floor augmentation. Methods: A 55-year-old, non-smoking woman presented with limited bone volume on both sides of the posterior edentulous maxilla that required rehabilitation. She had no systemic problems that might affect the surgical procedures. Preoperative cone-beam CT revealed significant maxillary sinus pneumatisation. Sinus lift procedures were performed on both sides of the maxilla, using a lateral surgical approach, and the maxillary sinuses were filled with a bovine bone graft substitute (BioOss[tm] small particles). A 25x25-mm collagen membrane (BioGide[TM]) was placed over the graft and the surgical flaps were sutured to entirely cover the membranes. Postoperative medications were amoxicyillin 500mg, clavulanic acid 125mg, ibuprofen 200mg and PerioGard[TM] rinse. Sutures were removed 14 days after surgery. Healing was uneventful, with no membrane exposure or other complications. After 12 months, further cone-beam CT showed significant gains in bone volume in both maxillary sinus areas, supporting the installation of osseointegrated implants. The patient postponed implant placement surgery; the left side was reopened 12 months after sinus lifting and the right side after 20 months. Before placing an implant, a bone biopsy was collected with a 2-mm trephine bur from both sides and samples were prepared for microtomographic and histological analysis. Results: Four months after implant installation, the healing abutments were connected and cone-beam CT was performed to evaluate the implants. Provisional prostheses were then installed and remained in function for 3 months, allowing functional analysis of the prosthetic rehabilitation. Definitive ceramic crowns were then installed. Microtomography showed newly formed bone (27%) and residual biomaterial (39%). Biopsy samples at 20 months post-operatively contained [ok?] 52% newly formed bone and 16% residual biomaterial. These results revealed the process of particle resorption and replacement by new bone tissue between 12 and 20 months. Histological analysis demonstrated remnants of biomaterial particles surrounded by newly formed bone without connective tissue. There were no signs of inflammation and there was no gap between the bone and Bio-Oss[tm] particles. The biopsy collected at 20 months showed noticeably fewer particles of residual biomaterial than that collected at 12 months. Conclusion: This report showed that an inorganic bovine bone graft associated with collagen membrane can be used successfully in this sinus lift procedure for the subsequent installation of dental implants. There was slow resorption of particles and continuous replacement by newly formed bone, which are desirable for to maintaining grafted bone volume for a longer period. It is important to emphasize that this report is not intended to change the protocol for installation of implants after sinus lifting using inorganic bovine bone and collagen membrane. The extended implant placement times (12 and 20 months) described here related to the patient's situation and are not necessary or desirable in clinical practice. -
Study Protocols: Maxillary Sinus Floor Elevation
based on the book chapter by Gustavo Avila-Ortiz andPablo Galindo-Moreno Summary This technique is used to gain bone height in posterior atrophic maxillary segments before implant placement. It is increasingly used in patients with maxillary sinuses that are too close to the upper jaw or excessive bone reabsorption from gum disease. Endpoints relate to the amount of new bone formation after grafting and survival of implants and implant-supported prostheses. and long-term success rates are high. It is also excellent for studying healing following grafting with different materials and regenerative strategies in large craniofacial defects. The protocol described here is based on a hypothetical study, and covers patient screening, selection, enrolment and randomization, including a sample size calculation (which is omitted in most published studies). There are multiple phases for planning and executing the sinus elevation, followed by post-operative evaluation, and further planning and placement of implants. Detail is given on the length and form of patient visits for evaluations using cone-beam CT, impressions, photos, clinical measures, bone biopsies and adverse events recording. The discussion is supplemented by images of bone core histology and diagrams of the paranasal sinuses, and the authors point out the difference between crestal and lateral approaches. The lateral approach is illustrated throughout, including follow-up at 24 weeks and implant placement. The authors also address the problems of membrane perforation and nasal meatus occlusion. Open full-text PDF (1.9 MB) -

Bone Spreading, Bone Condensing (Split Control System)
Streckbein, Roland -

Mandibular Distraction Osteotomy
Schleier, Peter / Schultze-Mosgau, StefanProcedure - Indications and preoperative planning - Incision technique and osteotomy - Placement of distraction apparatus - Wound closure and postoperative regimen Materials: V2-Alveolar distractor, Medartis (Switzerland) 2,0mm Screws for Osteosynthesis, Medartis (Switzerland) Vicryl Suture, Ethilon (USA) -

Sinus Floor Augmentation with Autogenous Chin Bone Grafts
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: In the maxillary incisor region, a sinus floor augmentation to enlarge the vertical bone supply may be indicated for a vertically reduced local bone height of less than 5 to 7 mm before procedures to rehabilitate masticatory function with an implant-bearing tooth replacement. For a single-sided deposit osteoplasty, the quantity of autogenous bone from the chin region is usually sufficient. The operative procedure of a single-sided lateral sinus floor augmentation is demonstrated with particulate spongious bone and alternatively with an autogenous block graft. The video also shows the operative method for a crestal sinus floor augmentation with the aid of the endoscopically controlled condensation technique. The advantages and disadvantages of the individual procedures are highlighted. In addition, the technique for harvesting chin bone transplants in different case examples is shown. Outline: - Operative technique for lateral sinus floor augmentation with autogenous particulate spongious bone - Operative technique for lateral sinus floor augmentation with autogenous block grafts - Crestal, endoscopically controlled sinus floor augmentation with condensation technique - Techniques for harvesting chin bone grafts - Range of indication for sinus floor augmentation - Lateral sinus floor augmentation - Operative technique of crestal, endoscopically controlled sinus floor augmentation - Operative technique of autogenous chin bone removal