







-


A SYSTEMATIC REVIEW OF RANDOMISED CLINICAL TRIALS USING CALCIUM SULPHATE AND DEPROTEINISED BOVINE BONE MINERAL (DBBM) VERSUS NATURAL HEALING FOR SOCKET PRESERVATION
Objectives: After tooth extraction, remodelling of alveolar bone takes place, as widely described in the literature. Significant dimensional changes occur in both soft and hard tissues, compromising future treatment of the edentulous area, but socket preservation may counteract this process. The aim of this review was to identify evidence related to the technique of socket preservation. Methods: An electronic search of MEDLINE–PubMed and Cochrane Central was performed. The inclusion criteria were based on the type of study, namely randomised controlled clinical trials and controlled clinical trials with natural healing as the control, published in English between 2000 and 2015. Results: The selection phase yielded 1138 suitable publications from MEDLINE–Pubmed and Cochrane Central, of which 38 were screened. After applying the inclusion criteria, 15 articles describing randomised controlled clinical trials were included in the study. Analysis of these showed that natural healing groups had a reduction in width of –0.16mm to –4.3mm and –0.56 to –3.75 in height. In the test group, results ranged from –2.5mm to +3.5mm for width and –2.48 to +1.3mm for height. Hence, the percentage of vital bone ranged from 25.7% to 57.4% at 6 months; for sockets filled with Bio-Oss[tm], this was between 10.4% and 34.5% at 6 months, and for sockets filled with calcium sulphate, between 36.25% and 63.16% at 3 months. There was insufficient evidence to establish the superiority of one biomaterial or technique above the other. Conclusion: According to analysis of the available literature, the alveolar preservation technique is associated with less vertical and horizontal bone loss than control methods. -

EARLY HISTOMORPHOMETRIC ANALYSIS OF EFFECTS OF CONCENTRATED GROWTH FACTOR ON BONE FORMATION IN EXPERIMENTAL BONE DEFECTS
Objectives: Concentrated growth factor (CGF) is a recently introduced platelet product that is gaining popularity, providing an innovative way to produce a fibrin matrix. Its clinical applications are now under investigation. The aim of this study was to assess the effect of CGF on new bone formation in a critical-size bone defect, alone and in combination with xenograft material. Methods: New Zealand white rabbits (n = 18; aged 16–20 weeks) were used. Two groups (n=9) were compared: in group 1, two critical-size defects were filled with CGF alone and CGF combined with xenograft material (BioOss[TM[); in group 2, two critical-sized defects were made, of which one was filled with xenograft material (BioOss[tm]) and one was left empty. Both groups were subdivided (n=3) for sacrifice after 15, 30 and 45 days. Under general anesthesia, two bone defects with a diameter of 3mm were made on the right tibia of each animal, and biomaterials were applied. CGF was obtained for each test subject by centrifuging 9 mL of intravenous blood in a Medifuge centrifuge . All defects were covered with titanium mesh membrane (Biohorizons[tm], USA). Tissue samples were stained with haematoxylin–eosin and analysed by optical microscope. Some sections were also stained with Masson’s trichrome. Data obtained from the study groups were evaluated statistically using one-way ANOVA and Kruskal–Wallis variance analysis, to investigate early bone formation, quality of newly formed bone, fibrosis, inflammation and vascularisation (with p Results: Histomorphometric analysis revealed no significant difference between defects 15 days after augmentation. CGF did not increase reossification, no inflammation was observed in any samples, and the degree of fibrosis and new bone formation were similar. There were also no significant differences after 30 days. CGF did not increase reossification significantly compared to other groups, no inflammation was detected, and the amount of fibrosis and new bone formation was similar. Good results were observed after 45 days, when the percentage of the newly formed bone, fibrosis, inflammation and new-bone quality were compared within all groups, but no significant difference were found between the biomaterials. Conclusion: We suggest that CGF does not induce bone formation in critical-size defects with a low regenerative capacity. This means CGF is less attractive alternative for reconstructing major bone defects in oral and maxillofacial surgery. Such bone defects might require more potent stimuli, such as a combination of functional biomaterials or autografts. -
RESTORATION OF THE UPPER NOSE DEFECT WITH NASAL PROSTHESIS—A CASE REPORT
Objectives: Surgical excisions of facial areas are often very difficult to rehabilitate. Defects in the maxillofacial region may be rehabilitated surgically or by prosthetic means to protect the defect from environmental conditions that may cause infection. Such defects are aesthetically displeasing and affect the social life of patients directly, therefore rehabilitation should be begun as soon as possible. The prosthesis increases quality of life, and allows adaptation to a social life. The aesthetic appearance is improved and preservation of the defect is achieved. Methods: An 81-year-old woman had a defect of the upper side of her nose caused by surgical intervention for a brain tumour. After the operation, surgeons were unable to restore the defect surgically due to her age and systemic condition. Thus the only choice for defect closure was an artificial prosthesis. Results: The patient had used cotton pads to cover up the defect before prosthetic intervention, which inevitably caused infections, but after placement of the silicone prosthesis the defect was healthy. Conclusion: Maxillofacial defects can be restored surgically, prosthetically, or both. Tissue engineering techniques are also available, but when the systemic condition of the patient is not suitable prosthetic techniques are the only choice, and these techniques should be improved. -

CYTOCOMPATIBILITY AND REGENERATIVE PROPERTIES OF SILVER NANOPARTICLE-COATED TITANIUM SURFACES
Objectives: Controlling oral biofilms by applying a metal nanoparticle coating is a very promising approach that relates to their potent antibacterial effect and superior impact on epithelial and connective tissue adhesion, leading to improved soft tissue regeneration. This study evaluated the antimicrobial effect and epithelial and fibroblast adhesion properties of silver nanoparticle-coated titanium surfaces, compared to untreated titanium and zirconia surfaces. Methods: To simulate abutment surfaces, disc-shaped samples were fabricated using zirconia, titanium, and titanium with a coating of nano-silver, deposited using splutter-coating technology. Three groups of samples were made and surface characterisation was carried out to assess surface morphology, thickness of the silver layer, and surface chemical content. To asses antimicrobial activity, samples in each group were placed in twelve- or twenty-four-well polystyrene culture plates and inoculated with bacterial cultures, and assessed for viable counts associated with the surface by obtaining total viable counts on TY/LB agar plates. Live and dead cells were quantified using a Backlight[tm] bacterial detection kit, and were imaged by confocal microscopy. To assess fibroblast adherence, oral fibroblasts were isolated from biopsy samples and grown in media (such as Dulbecco’s modified Eagle’s medium; DMEM) supplemented with serum and essential growth factors. Cells were added to achieve a density of 1 x105 cells/mL and placed in an incubator at 37° C and 5%carbon dioxide for 24 hours, to allow the cells to attach. Cell growth was assessed after 48 hours by MTT assay and compared to the control group. The amount of colour produced was directly proportional to the number of viable cells. All experiments were carried out in triplicates to negate any procedural error. Data were analysed by ANOVA with Duncan's multi-comparison procedure at a 5% confidence level. Results: Silver was deposited by sputtering silver ions on titanium surfaces, pretreated with emery paper and Piranha’s solution, to a final thickness of 6 mug/mm after 5 minutes. The silver ion release profile was studied over 28 days. The maximum cumulative silver concentration was 4 [mu]g/mL up to day 7 and thereafter underwent sustained release (with a similar rate to that of bioactive drugs from a matrix). Cytocompatibility assay showed time-dependant cell proliferation near the test samples that was inversely proportional to the amount of silver released. The silver-coated surfaces had a remarkable antibacterial effect against Staphylococcus aureus, Pseudomonas aeruginosa and Streptococcus mutans compared to untreated titanium and zirconia discs. The MTT assay revealed significantly higher fibroblast growth and proliferation in the presence of nanosilver-coated surfaces compared with untreated surfaces. Conclusion:Titanium surfaces can be modified by coating with silver nanoparticles using the sputtering technique. The modified surface show potent antibacterial action against a range of oral pathogens. Silver nanoparticle-coated surfaces may be used in regenerative therapy by virtue of their ability to promote increased adherence of gingival fibroblasts. -

SEQUENTIAL HEALING OF ONLAY BONE GRAFTS USING COMBINED BIOMATERIALS WITH CROSS-LINKED COLLAGEN IN DOGS
Objectives: The aim of this study was to observe the sequential healing of onlay grafts in terms of volumetric and histologic changes using different bone substances and absorbable membranes with and without collagen cross-linking. Methods: Onlay grafting with different materials was randomly assigned to both sides of the maxillae of 15 beagle dogs. There were four groups: no treatment (control group); bovine hydroxyapatite incorporated into a non-cross-linked collagen matrix (BHC) with non-cross-linked collagen membrane (NCCM) (group NN); BHC with cross-linked collagen membrane (CCM) (group NC); and porcine hydroxyapatite incorporated into a cross-linked collagen matrix with CCM (group CC). Radiographic and histological analyses were performed after three different healing periods: 4 weeks, 8 weeks and 12 weeks. Results: At week 4, the bone substances were well localised under the barrier membrane in groups NC and CC, but were spread out and flattened in group NN. Similarly, the mean augmented height was significantly greater in groups NC and CC (2.59 mm ± 0.42 and 2.43 mm ± 0.33, respectively) than in group NN (1.88 mm ± 0.29; p Conclusion: Combining a biomaterial with cross-linked collagen might contribute to maintaining its initial morphology, with excellent biocompatibility in early healing period of lateral onlay grafts. -
APPLICATION OF DENTAL IMPLANT TREATMENT FOR AESTHETIC AND FUNCTIONAL REHABILITATION OF ALVEOLAR CLEFT PATIENTS
Objectives: Patients with cleft lip and palate (CLP) frequently have a missing incisor at the alveolar cleft site. Owing to recent advances in secondary bone grafting (SBG) techniques, dental implant treatment has become an acceptable method for restoring the edentulous space at the cleft site in addition to conventional methods using bridges or dentures. In this study, we investigated the risk factors related to aesthetic outcomes of implant treatment at alveolar cleft sites. Methods: A total of 13 patients (8 women, 5 men) treated with implants for missing teeth associated with an alveolar cleft at the Implant Clinic of the Dental Hospital at Tokyo Medical and Dental University between 2002 and 2010 were examined. The patients’ genders, cleft types and number of dental implants were recorded as well as their ages at bone grafting for cleft closure, at additional bone grafting prior to dental implant surgery, and at dental implant placement. Three patients had a bilateral and ten had a unilateral cleft lip, alveolus, and palate. Sixteen dental implants were evaluated. Risk factors such as lip line, length from the nasal floor to the alveolar ridge, width of the edentulous span, gingival margin of the adjacent teeth, and cleft types (bilateral or unilateral) were designated as either high risk or low risk. Results: Neither dental implant loss nor bone resorption around the dental implants were observed 5 to 13 years after final restoration. All patients were satisfied with the aesthetic and functional outcomes of the treatment. All except underwent bone grafting to close the alveolar cleft with autologous cancellous bone harvested from the iliac crest (SBG) between the ages of 11 and 28 years. Two underwent additional bone grafting prior to implant placement. Their ages ranged from 18 to 36 years (mean 23 years) at the time of placement. In 11 patients, dental implants were installed at least 6 months after the last bone grafting at the cleft sites. One patient did not undergo any bone grafting before implant surgery, and one had an implant installed 5 months after the last bone grafting. Two cases with only low risk factors had good aesthetic outcomes from implant treatment. Out of the remaining cases, eight had one high-risk factor, one had three high-risk factors, and two had four high-risk factors at the time of placement. Although the aesthetic outcomes of those with one high-risk factor were slightly inferior to those with no high-risk factors, they were nonetheless satisfactory. The value of aesthetic outcomes was not varied among the different types of risk factors. In contrast, the aesthetic outcomes of the groups with three and four high-risk factors were inferior to those of the other groups. Conclusion: The results suggest that if bone grafting is performed appropriately, treatment using dental implants could be effective for patients with alveolar clefts. However, compared to normal jaws, cleft jaws required more complicated implant treatment and aesthetic outcomes are more variable. To overcome the clinical limitations, it is important to consider and screen patient risk factors to achieve favourable outcomes. The study suggests that aesthetic outcome may depend on the number of risk factors present, rather than on the presence of a specific high-risk factor. The two patients with no high risk factors had a high-risk factor earlier (edentulous span width), which was corrected by orthodontically before implant surgery. Thus, it is important to reduce the number of high risk factors to obtain good aesthetic outcomes in dental implant treatment of alveolar cleft patients. -

EFFECT OF HYDROPHILIC GEL COMPLEX MADE FROM EXTRACT OF ALOE VERA AND CURCUMINOID ON BONE CELL PROLIFERATION
Objectives: The objective of this study was to evaluate the influence of direct exposure of prepared hydrogel on machine-surfaced titanium discs compared to that of non-hydrogel discs on the bioactivity of UMR106 cells. Methods: To determine cell viability, an MTT assay was conducted using 10,000 cells per cm2 seeded into twelve-well plates containing gel-coated and non-gel-coated discs and F12K medium with 20% fetal calf serum (FCS) and 100μg/g streptomycin. The cell medium was changed once a week during the experiment. After 24 hours and 7, 14 and 21 days, MTT solution was added to the medium. The cells were then incubated in the dark for 4 hours at 37° C. The MTT assay was performed on the discs that were not seeded with the cell culture, in order to exclude the effect of the material on the results, as distinct from the cells’ reactions. Cell morphology was studied by inverted light microscopy using a Leica microscope (090-135.002) equipped with a Nikon[tm] Ds-Fil digital camera. Alkaline phosphotase (ALP) content was determined to reveal changes in differentiation of bone-forming cells caused by the test substance SensoLyte[tm] (p-nitrophenyl phosphate (PNPP). The ALP assay was run after 24 hours and 7, 14 and 21 days of culturing in Dulbecco’s modified Eagle’s medium (DMEM), with low glucose, l-glutamine, 10% FCS, 100 U/mLof penicillin, 100μg/g streptomycin, 0.1μm dexamethasone and 0.005μm ascorbic acid. Transmission electron microscopy (TEM) of UMR106 cells in chamber slides were incubated with titanium discs for 7 and 21 days. Results: Values from the MTT assay were tabulated, and the average of three duplicates was determined for all batches incubated for 24, 48 and 72 hours. Cell viability was greater at 72 hours (1.030% for disc 1, 1.016% for disc 2 and 1.021% for disc 3). The cell viability for disc 1 was 69.038% at 24 hours, 76.028% at 48 hours and 91.875% at 72 hours. Values for disc 2 were 71.931% at 24 hours, 84.727% at 48 hours and 90.621% at 72 hours. For disc 3, they were 70.923% at 24 hours, 84.932% at 48 hours and 91.038% at 72 hours. Conclusion: The effect of the formulated hydrogel gel increased the wettability of the titanium discs and showed significantly good cell viability and osteoblastic cell proliferation. This suggests that the hydrogel is associated with early bone healing and bone remodelling. -

ALVEOLAR RIDGE PRESERVATION WITHOUT BARRIER MEMBRANE—A CASE SERIES
Objectives: Alveolar ridge preservation (ARP) is pre-implant surgery that minimises alveolar ridge resorption after extraction. It involves grafting a socket with bone or biomaterials with or without barrier membrane (BM). Many guidelines suggest applying a combination of bone graft and BM, but some systematic reviews point out that the available evidence is too weak to justify the use of BM. The aim of this study was to observe the outcomes of ARP without BM in the premolar and molar region. Methods: This study included five systematically healthy patients including (1 man; 4 women; mean age 55.4 years). Their premolars or molars were irrational to treat because of severe periodontitis or large tooth defects and periapical disease. Bone volumes were measured before surgery using cone beam CT (CBCT). All extractions were performed with flap formation to remove the inflamed tissue under local anesthesia. Sockets were rinsed and curetted with alveolar curettes, before grafting with deproteinised bovine bone (BioOss Collagen). Once the extraction socket was grafted, the preserved site was directly sutured without any application of barrier membrane. After 6–9 months of healing, bone volumes were re-evaluated by CBCT. Four measures were recorded for all preserved sites before and after treatment. Horizontal volumetric changes were measured at three levels (3mm, 5mm and 7mm below the most coronal aspect of the bone crest) and marked as level I, II, III respectively, while the vertical dimensional changes were assessed by measuring the palatal and buccal wall peaks (marked as level IV). Resorption rates were calculated by the formula: Resorption rate (%) = (length of alveolar bone before extraction – length of alveolar bone after alveolar ridge preservation/length of alveolar bone before extraction x 100. The resorption rate and reduction of alveolar ridge was recorded for each level . Results: No postoperative complication occurred at any site.The resorption rates and reduction of alveolar ridge for every patient in level I, II, III and IV were recorded. The mean resorption rate and amount of reduction were14.4% and 1.4mm for level I,10.6% and 1.2mm for level II,8.4% and 0.8mm for level III,and 4.6% and 0.6mm for level IV, with a mean healing time of 7.4 months. Compared with the average bone resorption rate (25–30% in the first 6 months) and amount of reduction (3.8mm horizontally, and 1.24mm vertically in the first 6 months) of natural healing, the efficacy of ARP without BM is still satisfactory in terms of maintaining bone volume after extraction. Adequate bone width and height were obtained after ARP. Radiolucent areas of periapical disease or periodontitis were also well regenerated with bone tissue. In the subsequent implant placement procedure, a wide buccolingual osseous table with commendable bone quality was observed after re-entry. Conclusion: ARP using bone substitute materials alone, without BM coverage, is effective for maintaining bone volume, but cannot stop bone resorption. Further well-designed clinical trials are needed to evaluate the efficacy of BM. -
IMPACT OF ATTACHMENT TYPE ON IMPLANT SURVIVAL OF IMPLANT-SUPPORTED PROSTHESES IN THE PATIENTS WITH MAXILLARY RESECTION—A CASE REPORT
Objectives: Oral implants have a very important role in restoring loss of retention and stability. The most important problem is resorption of the bone surrounding implants which occurs because of excessive lateral forces on the prosthesis. Choosing the right attachment type minimises the “overturning moment” on the defect and is very important for implant survival. The purpose of this study was to select a suitable attachment type for a patient with implant-supported prostheses for a maxillofacial defect. Methods: The patient had a palatal defect that was restored surgically after tumour surgery with mucosal graft. Two implants with ball attachments were inserted in the left region of the maxilla due to retention and stabilisation problems with the prosthesis. Resorption of bone surrounding the implants and clinical condition of the prosthesis were followed up. Results: No bone resorption around the implants was observed during 15 years of follow-up. Conclusion: The design of the implant-supported prosthesis has a major role in the long-term survival of implants. The attachment type affects the lateral forces that cause overturning moments on the prosthesis. Locator, era and ball-type attachments, as used in the present case, have a positive impact on long-term success. -
ALTERNATIVE TECHNIQUE FOR RETAINING FRACTURED BALL ABUTMENTS TO EXISTING MANDIBULAR OVERDENTURES—A CASE REPORT
Objectives: Complications with implant prosthesis have been categorised as surgical complications, implant loss, bone loss, peri-implant soft tissue complications, mechanical complications and aesthetic complications. Fractures of implant components, especially abutments, may occur due to fatigue from biomechanical overload, improper placement techniques or manufacturing errors. The aim of this case report is to present a useful technique in cases in which ball abutments are fractured and unable to be removed. Methods: A 49-year-old woman presented to the department of Prosthodontics at Istanbul University. She had been wearing a maxillary complete denture and a mandibular overdenture supported by two implants for 5 years. She complained about the loss of retention of the lower overdenture. On clinical evaluation, we discovered that one of the ball abutments was fractured and therefore retention was lost. We tried to remove the fractured abutment from the implant body using a Straumann service set and a conventional method, but the result was unsatisfactory and the fractured abutment could not be recovered. Therefore a new technique was attempted without removing the implant body. Results: At the 6-month follow-up, radiological and clinical examination revealed no problems in the marginal bone around the implant and soft tissue. Conclusion: This technique appeared successful and avoided the use of invasive surgical methods. -
COMPARATIVE EVALUATION OF SIMULTANEOUS MAXILLARY SINUS FLOOR ELEVATION AND IMPLANT PLACEMENT WITH AUTOGENOUS BONE VERSUS A BOVINE-DERIVED XENOGRAFT—A 6-YEAR RETROSPECTIVE STUDY
Objectives: The long-term outcome after simultaneous maxillary sinus floor elevation and implant placement with autogenous bone or bovine xenograft was explored. Methods: Simultaneous maxillary sinus floor elevation and implant placement with autogenous bone or bovine xenograft (BioOss) was assessed in 45 patients with vertical maxilla dimension ofless than6mm. Sinus augmentation was performed using mandibular bone grafts or BioOss. In the autogenous bone group, 56 implants were placed in 21 patients, while in the BioOss group, 24 patients received 62 implants. After 72 months of functional loading, implant survival and reduction in augmentation height were compared between the groups.Fisher's exact test and equivalence testing were used to compare implant survival rates. Results: An overall survival rate of 95.7% was found for implants 6 years after insertion. In the autogenous bone group, the implant survival rate was 96.4%, while in the BioOss group, it was 95.2%. The difference was not statistically significant (p > 0.05); both treatments were equivalent (confidence interval 90%) for the equivalence interval (–0.1; 0.1), and 46.3% of cases showed no reduction in the augmentation height at 6 years follow-up, when augmentation was performed with autogenous bone; in the BioOss group, no resorption was found in 50.8% of the augmented areas. A reduction in augmentation height of up to 25% was found in 44.4% in the autogenous group, and of 42.4% in the BioOss group. In 9.3% of all cases in the autogenous bone group and in 6.8% in the BioOss[tm] group, up to 50% of the augmented height was resorbed. Conclusion: After a 6-year evaluation period, the use of BioOss for the maxillary sinus augmentation seems to be equivalent to autogenous bone grafting. -
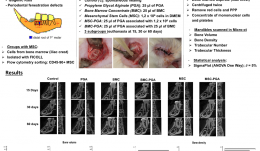
MICRO-TOMOGRAPHIC EVALUATION OF BONE MARROW MESENCHYMAL STEM CELLS AND BONE MARROW CONCENTRATE IN PERIODONTAL REGENERATION
Objectives: The study aimed to evaluate bone formation in periodontal fenestration defects in rats, using bone marrow mesenchymal stem cells (MSCs) or bone marrow concentrate (BMC) with propylene glycol alginate (PGA) as a vehicle. Methods: Periodontal fenestration defects (2mm high x 4mm wide x 1mm deep) were created in the mandible of isogenic rats. The animals were allocated into six groups and further divided into three subgroups for euthanasia at 15, 30 or 60 days postoperatively (n=6 in each subgroup). The control group (C group) was the spontaneous healing group. The PGA group received 25 µl of PGA as vehicle. For the MSC group, stem cells were collected from the iliac crest of two isogenic rats, isolated with Ficoll and cultured in flasks and separated by flow cytometry to obtain a CD45-90+ cell population. In the MSC group, a pellet containing 1.2 x 106 cells was applied to each defect. In the MSC-PGA group, 25 µl of PGA was added to the same pellet. In the BMC groups (BMC and BMC-PGA), 1 mL of bone marrow from iliac crest was aspirated immediately before surgery and was centrifuged twice to remove red cells and poor platelet plasma, producing a concentrate of MSCs and platelets. The BMC and BMC-PGA groups received 25 µl of BMC, but in the latter it was mixed with 25 µl PGA. After euthanasia, mandibles were fixed and scanned by computer microtomography. Bone volume, density and trabecular number and thickness were analysed by SigmaPlot™. The normality of the data was checked and one-way ANOVA used with a significance level of 5%. Results: Bone volume was increased in all groups and at all-time points (p 0.05), except the PGA group which was lower (p 0.05). At 30 days, trabecular thicknesses for MSC and MSC-PGA were similar (p > 0.05) and both were higher than the other groups (p Conclusion: Overall, the stem cells in the proper vehicle resulted in faster and more extensive bone regeneration in periodontal fenestration in rats. MSC alone and BMC in the vehicle were also associated with better bone regeneration than spontaneous healing or vehicle alone.

Take this survey to help us improve your experience
on Dental Campus
For completion, you get 3 days unlimited access to:
- All lectures
- All cases
- All videos