







-


AZITHROMYCIN-RELEASING POLYMERIC MEMBRANES FOR GUIDED BONE REGENERATION (GBR)
Objectives: The objective of this study was to develop and evaluate a calcium phosphate-coated polycaprolactone (PCL) electrospun membrane loaded with azithromycin, in order to make use of the antimicrobial and anti-inflammatory properties of the antibiotic in GBR. Methods: PCL membranes were fabricated via solution electrospinning. Azithromycin at three different doses (1mg, 2.5mg and 5mg) was dissolved in ethanol (100%) and loaded onto the PCL- and calcium phosphate (CaP)-coated membranes. The membrane discs were soaked in the antibiotic solution for 8 hours befor evaporating off the solvent at room temperature. The release profile at different azithromycin concentrations was evaluated by colorimetric assay. Membrane surface morphology was assessed using scanning electron microscopy, surface area analysis for surface area and porosity, and electrokinetic analysis for surface charge. Chemical composition was determined by X-ray diffraction. Antimicrobial activity in vitro was determined by disk diffusion for up to 14 days. In vivo analysis was carried out by applying the membranes to critical size calvarial defects (5mm diameter) in Sprague Dawley rats. Bone formation was assessed by micro-CT, histology and histomorphometry. Results: Azithromycin was successfully loaded onto PCL/PCL-CaP membranes with a high loading efficiency of up to 85%. The release profile showed rapid release of the drug within the first 24 hours, followed by linear release over the next 14 days. The release profile was similar for all doses, but the amount released in both initial and late stages was significantly affected by the initial dose: for the 1-mg dose, 80% of the drug was released at 24 hours, with total release after 14 days; the higher doses (2.5mg and 5mg) showed 20% and 50% release at 24 hours and 14 days respectively. This controlled and sustained release of azithromycin was able to inhibit bacterial growth in vitro for up to 14 days. Application of azithromycin-loaded PCL-CaP membranes in rat calvarial defects demonstrated improved bone regeneration after 8 weeks of implantation for antibiotic-loaded membranes compared to unloaded controls. Conclusion: Hydrophobic azithromycin was successfully encapsulated on to PCL/PCL-CaP membranes using an ethanol evaporation technique. Excellent encapsulation efficiency was observed, along with a controlled-release profile and efficient antibacterial properties. The azithromycin-loaded membranes showed enhanced bone formation compared to unloaded controls. These results suggest that azithropmycin-loaded membranes have both osteogenic and antimicrobial properties that may be clinically useful for enhancing GBR procedures. -

THE USE OF BIOACTIVE GLASS AS BONE SUBSTITUTE IN ORAL IMPLANTOLOGY—A CASE SERIES
Objectives: The aim was to present our patient experiences and clinical outcomes following the use of bioactive glass bone graft material (Leonardo[tm]) in various dental implant procedures. Methods: The procedures included alveolar ridge splitting, immediate implant placement, sinus lifting, cyst removal and bone grafting followed by implant placement and management of a bone defect around the implant in the aesthetic zone. Results: All patients tolerated these procedures well and had no postoperative complications. The clinical and radiological results were satisfactory. Conclusion: Despite the limitations of this case series, synthetic bioactive glass is a promising material for improving therapeutic outcomes in dental implantology. -

THE INFLUENCE OF PIEZOSURGERY ON BONE HEALING AROUND TITANIUM IMPLANTS – A HISTOLOGICAL STUDY IN RATS
Marcelo Sirolli(Brazil), Carlos Eduardo Secco Mafra, Rodrigo Albuquerque Basílio dos Santos, Luciana Saraiva, Marinella Holzhausen, João Batista César Neto Objectives: The aim of this study was to investigate the influence of two techniques for dental implant site preparation on bone healing around titanium implants. Methods: Fifteen male Wistar rats (weighing approximately 300g) were used. Tibias were randomly assigned to undergo implant site preparation with a conventional drilling technique (control group) or piezoelectric device (piezo group). After 30 days, they were sacrificed and the following histomorphometric parameters were evaluated separately for cortical and cancellous tibial regions: proportion of mineralised tissue (PMT) adjacent to implant threads (500μm adjacent); bone area within the threads (BA); and bone–implant contact (BIC). Results: There were no differences between the two groups for cancellous BIC (p>0.05) and cortical PMT (p>0.05). A higher mean percentage of BA was observed in the piezo group in cortical regions (controls 71.50% ± 6.91 and piezo group 78.28% ± 4.38; pin cancellous regions (controls 9.35% ± 5.54 and piezo 18.72% ± 13.21; p Conclusion: Within the limits this study on implant site preparation, we conclude that piezosurgery favours bone healing rates in cancellous bone regions, while the drill technique gives better results in cortical regions. -

126 ANTERIOR DENTAL ROOT FRACTURES—PRESERVATION OF THE ALVEOLAR RIDGE USING IMMEDIATE IMPLANT PLACEMENT
Objectives: The aim of this study was to evaluate clinical treatment of immediate dental implant placement of root fractures in adult patients following dentoalveolar trauma. Methods: A descriptive study was performed for cases of root fractures by systematic review of the digital records of all patients with dentoalveolar trauma and root fractures between May 2009 and May 2010 at the Unit of Oral and Maxillofacial Surgery, Hospital Clínico Mutual de Seguridad C.Ch.C., Santiago de Chile. Results: A total of 894 dentoalveolar trauma cases were identified, of which 56 (6.3%) were root fractures. In terms of outcome, implants had a 98% success rate, with no complications associated with vestibular bone loss or gingival unaesthetic recession. Conclusion: We believe that immediate replacement of lost teeth after root fractures with dental implants is a reliable option for patients with dental trauma, with no vestibular bone loss complications in the short term. -
THE FATE OF BUCCAL BONE AROUND DENTAL IMPLANTS—A 12-MONTH POST-LOADING FOLLOW-UP STUDY
Objectives: Buccal bone thickness is considered to be an important factor during implant surgery. Its resorption might have an effect on soft tissue stability and eventually on implant survival. This study aimed to investigate the resorption of buccal bone during the first 12 months after implant loading. Methods: The study included 24 patients (47 implants). Buccal bone thickness was measured during implant surgery at several distances from the implant shoulder using a specifically designed device that allows bone thickness measurements without requiring elevation of a mucoperiostal flap. The measurements were repeated after 12 months of loading. Sixteen implants were placed flapless and 31 with the elevation of a flap. Of the latter, 19 were placed following a one stage protocol and 12 following a two-stage protocol. Results: The mean reductions in buccal bone thickness, when all groups were pooled, were 0.26mm,0.36mm,0.35mm and 0.27mm at the shoulder, and 2mm, 4mm and 6mm apically. Implants with initial bone thickness of Conclusion: Various authors have claimed that an initial buccal bone thickness of 2mm is necessary for preservation of the buccal bone plate. It was hypothesised that thin buccal plates are less resistant to different types of trauma that implants can endure and are therefore more prone to resorption and buccal implant exposition. Within the limitations of this study, one might question the necessity of having a thick bone plate at the vestibular site of the implant. -
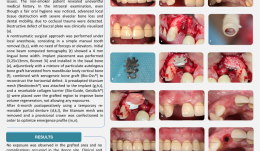
GUIDED BONE REGENERATION (GBR) IN THE AESTHETIC ZONE—RESTORATION OF HORIZONTAL BONE DEFECTS WITH MIXED BONE GRAFT AND TITANIUM MESH
Objectives: To report a case of a severe horizontal defect in a maxillary lateral incisor in which GBR was applied with adjunctive use of autologous (mandibular body cortical) bone and xenogeneic bone graft (BioOss[TM]), combined with titanium mesh, to improve clinical and aesthetic effectiveness, with a two-year follow-up. Methods: A 30-year-old non-smoking female patient with an uneventful medical history was referred to the Implantology Clinic at Paulista University, São Paulo, with a compromised maxillary lateral incisor, and complaining of masticatory parafunction and aesthetic issues. Despite satisfactory oral hygiene, intraoral examination showed advanced local tissue destruction with severe alveolar bone loss and dental mobility. A large buccal plate dehiscence was detected clinically and radiographically. A non-traumatic surgical approach under local anaesthesia consisted of simple manual tooth removal, requiring no forceps or elevators. After 30 days of healing, a cone beam CT showed lingual bone width of 3mm. An implant (3.25 x 13mm Biomet-3i) was installed in the basal bone adjunctively with a mixture of particulate autologous bone graft harvested from mandibular body cortical bone and BioOss[tm] xenogeneic bone graft (to reconstruct the horizontal defect). A preadapted titanium mesh (Neobiotech[TM]) and resorbable collagen barrier (BioGide[TM]) were placed over the grafted region to help maintain bone volume and prevent any exposures. During a six-month healing period, the patient used a provisional removable partial denture. Then the titanium mesh was removed and a provisional crown was fabricated to optimise the emergence profile. Results: No bone exposure was observed in the grafted area and no complications occurred in the donor site. Postoperative clinical and CT examinations at 6, 12 and 24 months showed sufficient and satisfactory bone formation. Besides the limited torque (15N/cm) during implant placement, the final prosthetic design was successful. At two-year follow-up, volumetric stability and satisfactory functional and aesthetic results were achieved. Conclusion: Mixed bone grafts combined with titanium mesh appear to be an effective and advantageous procedure for horizontal bone defects in aesthetic zones, providing volumetric stability and satisfactory functional and aesthetic results. -
HOW DEEP DOES SUBGINGIVAL IMPLANT SURFACE AIR-POLISHING REACH AND WHAT INFLUENCES CLEANING EFFICIENCY? AN IN VITRO STUDY ON TITANIUM DISCS
Objectives: Recent studies show that air-polishing is an effective method for maintaining implants and treating peri-implant mucositis and peri-implantitis. However, none of the studies investigated how the method works, in terms of the shape and size of the cleaning area around the nozzle, the influence of different settings and depth of pockets. This study aimed to identify the most effective technique by examining the most important parameters. Methods: Forty-eight titanium SLA surface discs were coated with calcium phosphate (CaP) to simulate visually identifiable plaque and were inserted in subgingival models. All applications were done using an EMS Air-Flow[tm] master with a plastic Perio-Flow[tm] nozzle, on Perio Mode and using EMS Air-Flow[tm] Plus Powder. In the first part of the experiment, discs were treated with the EMS airflow device for 5 seconds in a static state using different air and water settings, nozzle depths and chambers with different powder flows. The most effective settings, established from these results, were used for the second part of the experiment, but the nozzle was moved in three different ways. In both parts, powder consumption, water consumption and total cleaned area were calculated. In the first part, the analysis was carried out using a multifactorial (25 factors) statistical design (ANOVA). The assumption was checked graphically with a Q-Q plot and tested with Levene’s test. Only factors with p Results: The average powder consumption for a standard chamber (EMS Air-Flow[tm] Perio Plus Chamber) with low-pressure settings was 0.05 gr and 0.13 gr with high pressure. The factors that significantly influenced cleaning efficiency were air pressure, powder flow, the combination of air pressure and powder flow, the combination of air pressure and nozzle depth, and the combination of the water volume and powder flow. Factors were considered relevant with a p2) of the model statistical model was 85.63%, meaning that 85% of the results could be explained by these factors. The air pressure had a major effect. The total cleaned surface area was greater in all higher-pressure groups. The cleaning effect was spread around the nozzle, whereby the size of the cleaned area exceeded the nozzle’s physical borders both horizontally and vertically. The mean distance between the right edge to the left edge of the cleaned area was 6.53mm at high pressure and 4.35mm at low pressure. The cleaning effect reached an average of 2.8mm beyond the nozzle exit (i.e. the nozzle cleaned vertically deeper than its own size). There were no significant difference between the three nozzle movements, but cleaning efficiency decreased significantly if there was no movement or powder, while the presence of powder and any type of movement had a big impact on cleaning efficiency. Conclusion: The study unravelled how air-polishing works on implant surface, thus cleaning efficiency can be improved by paying attention to the factors outlined here, the most important of which is air pressure. The more pressure applied, the better the cleaning effect. Inserting the nozzle into deeper pockets enhances the effect, and moving the nozzle is crucial. Clinicians should use high-pressure settings, preferably in deep pockets, with nozzle movement. Certain areas were only cleaned superficially after 5 seconds, therefore we recommended applying airflow twice for 5 seconds per site for deeper cleaning of implant surfaces. Another important finding is that cleaning extends beyond the nozzle end, confirming that it is better at reaching deeper areas than hand devices. -

BONE AUGMENTATION IN HIV-POSITIVE PATIENTS ON HIGHLY ACTIVE ANTI-RETROVIRAL THERAPY—CASE REPORTS AND REVIEW OF THE LITERATURE
Objectives: The aim of the study was to report two clinical cases of HIV-positive patients on highly active anti-retroviral therapy (HAART) who received implant-supported rehabilitation after bone reconstruction procedures and were followed for up to 10 years. Methods: Case 1 was a 44-year-old women who was referred to treatment because of persistent symptomatic apical periodontitis in elements #30 and #29. During exploratory endodontic surgery, in an attempt to retain her teeth, a longitudinal fracture and extensive bone dehiscence were detected in #29 and replacement by dental implant was planned. Viral load was undetectable and CD4/CD8 counts were compatible with an immunocompetent condition. In a second event, tooth #29 was extracted and the large bone defect filled with a mixture of autogenous bone plus bovine hydroxyapatite. A collagen membrane was used as a barrier. The implant was placed, and after the osseointegration period a metal–ceramic crown was installed. The 10-year follow-up appointment and control x-rays showed healthy and stable peri-implant tissues. Case 2 was a 47-year-old man who was referred for replacement of an upper molar with severe bone loss and close relation with the pneumatised sinus. He had been on HAART for approximately 8 years. Viral load was undetectable and the patient was considered able the receive the intervention. The tooth was extracted and socket preservation techniques were used (bone substitute plus collagen membrane). After healing, a sinus lift procedure was performed with the lateral window technique, using bovine hydroxyapatite and collagen membrane. The implant was placed at the same time. The patient healed uneventfully and has been followed for 8 years with good results. Results: Both HIV-positive patients undergoing HAART had undetectable viral loads and white cell counts (CD4/CD8) within a range that is compatible with dental interventions. Both received antibiotic cover with amoxicillin 500mg and clavulanic acid 125mg three times daily for one week to prevent postoperative infection. They were prescribed ibuprofen 600mg three times daily to control postoperative discomfort. Both patients were followed by an assistant physician who allowed them to undergo the planned dental intervention. All the interventions healed uneventfully and both patients were able to receive the prosthesis within the planned treatment period. At biannual follow-up in a periodontal maintenance program, implants were functional, without clinical or radiographic signs of peri-implantitis or mucositis. The patients maintained satisfying levels of oral hygiene and did reported no significant systemic alterations. Both had undetectable viral loads and good CD4/CD8 counts. Conclusion: HIV-positive patients undergoing HAART are usually able to maintain good systemic conditions and therefore may be eligible to receive implant-supported restorations. In both cases presented, follow-up showed stable and healthy peri-implant tissues and functional implants. Literature on this topic is still restricted to few studies with small samples, but previously published data suggest that well-controlled HIV-positive patients can benefit from dental implants, even when bone augmentation procedures are needed. The need for antibiotic coverage is still controversial. -
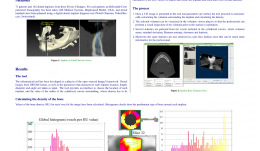
DEVELOPMENT OF A HELICOIDAL CT-BASED COMPUTER TOOL TO ESTIMATE BONE DENSITY AROUND DENTAL IMPLANTS
Objectives: The study analysed dental images from DICOM (digital imaging and communications in medicine) formats in order to establish the volume of a cylindrical corona around and along the implants, to calculate statistical values of bone density for each slice of the corona (and for total volume), and to determine a global value based on a mathematical formula that determines a unique density value. Methods: The study included 71 patients from three private clinics, each of whom underwent helicoidal CT, to obtain dental images in DICOM format. A total of 162 dental implants were planned using a digital dental implant diagnosis tool to create files in a specific format. These were analysed using a Nobel Clinician Viewer[tm] program. Results: This computer tool was developed as a plug-in of the open sourced ImageJ framework. The inputs are dental DICOM images from helicoidal CT, and parameters that characterise each implant from Nobel Clinician planifications are location, length, diameter and angle. The tool provides an interface for selecting the location of each implant, and the value of the radius of the surrounding cylindrical corona, from which density will be calculated. It also allows import and export of implant data to and from an external database. Once a 3-D image is presented to the tool and parameters are settled, the tool proceeds to automatically calculate the volume surrounding the implant and its density. The selected volume can be visualised in the plug-in for inspection prior to statistics export. Several statistics are gathered from the voxels in the cylindrical corona, including whole volume mean, standard deviation, Shannon entropy, skewness and kurtosis; these can be much more informative if retrieved per slice. Finally, a mathematical formula of bone density has been developed. Conclusion: The tool presented here allows automatic calculation of density of the bone surrounding dental implants. In the future we plan to use data-mining techniques on the clinical data of these 71 patients to establish predictive models of implant stability and subsequent success rates of dental implants. -

DIGITAL IMPLANT PLANNING WITH 3-D PRINTERS AND CBCTS IN GUIDED SURGERY AND BONE GRAFT PROCEDURES
Objectives: Here we present a new digital implant planning protocol using 3-D printing, cone beam CT (CBCT), scanners and computer-assisted design software. Biomodels and surgical guides are manufactured with 3-D printers and digital planningis used to allow implant placement based on the concept of prosthetically driven implantology. Methods: The digital implant planning protocol with 3-D printers is based on the premise that digital files obtained from CBCTs and scanners can be imported to computer-assisted design (CAD) software and all phases of the treatment can be performed virtually, before implant surgery. First, CBCTs from the areas of interest are obtained. A set of frontal photographs are taken and the teeth are scanned with intra-oral scanners (impressions can be taken and scanned if an intra-oral scanner is not available). The digital CBCT files are converted from DICOM (digital imaging and communications in medicine) to stereolithography (STL) files using open-access software and imported to CAD software. Images are edited using the principles of digital smile design, and a digital wax-up is produced. Digital planning allows all the images to be overlaid (CBCT; scanned teeth plus gingiva; digital wax-up; photos) so that implant positions can be planned with all the references needed with respect to prosthetically driven implantology. When digital planning is finished, polylactic acid biomodels can be printed by 3-D printers, reproducing the area to be operated. Biomodels are particularly useful in cases where large bone defects will be grafted, because the surgeon can plan the bone reconstruction procedure and adapt bone blocks and titanium meshes more easily. Surgical guides are also printed and used to drive the burs during surgery. Three cases are described. Results: The first case was a young patient who had suffered a car accident and lost the upper incisors. Orthodontic treatment was used to obtain an ideal mesiodistal space for implant placement and a fixed bridge supported by two implants. After orthodontics, CBCT showed that bone reconstruction was needed and autologous bone grafts were planned. A biomodel was printed by 3-D printer and used to help adapt the block before elevating the flap in the area receiving the graft. After 4 months, another CBCT was obtained and the implant position was digitally planned based on the virtual wax-up. Implants were successfully placed and a fixed bridge with ceramic gingiva was built. The second case was an elderly patient who needed implant surgery for placement of two implants to support a fixed bridge. The patient already had implants on the posterior mandible and on the right central incisor. After digital wax-up and CBCT evaluation, two implants were placed and the bridge was successfully built. The third case was another young patient who needed orthodontics before surgery for single implant placement. Every step of the planning protocol was followed and the implant was placed in the predetermined position. All cases healed uneventfully and were followed up for two years or more. Conclusion: The digital implant planning protocol appears to be a feasible and affordable treatment for oral rehabilitation. It allows surgeons and restorative dentists to preview the desired results and study cases in a very detailed manner, by overlaying different images providing precise information about the relation between the teeth, gums, bone and face. The software is open-source and the 3-D printers are low-cost and use affordable polymer feedstock, so this protocol is a useful tool with an excellent cost–benefit ratio. To the best of our knowledge, we are the first to use low-cost domestic 3-D printers to manufacture biomodels and surgical guides. Case–control multicentre studies will be useful for validating the protocol and comparing the accuracy of less expensive polymer-based 3-D printers with larger, expensive industrial printers. -
RIDGE PRESERVATION OF MAXILLARY THIRD MOLAR POST-EXTRACTION SOCKETS USING A NOVEL PLGA/HA SCAFFOLD, WITH AND WITHOUT SIMVASTATIN—AN 8-MONTH CLINICAL FOLLOW-UP OF A HUMAN SPLIT-MOUTH RANDOMISED CONTROLLED CLINICAL TRIAL
Objectives: This study aimed to evaluate the osteoinductive capacity of Simvastatin[tm] incorporated into a poly(lactide-co-glycolide)/hydroxyapatite (PLGA/HA) scaffold and possible inflammatory reactions associated with its use. For comparing bone formation, a positive control group with xenogeneic bovine bone graft material (BioOss Collagen) and a negative control with no graft were used. This was a split-mouth randomised controlled clinical trial. Methods: This research was conducted in 13 patients requiring bilateral extraction of maxillary third molars at the Federal University of Santa Catarina. After extraction, different biomaterials were placed for regeneration of the extraction zone, with randomly assignment of four treatment modalities: Group 1 (negative control), not filling (clot); group 2 (positive control), BioOss Collagen; group 3 (test), PLGA/HA; group 4 (test), PLGA/HA plus Simvastatin[tm] at a concentration of 2.0%. PLGA/HA and PLGA/HA plus Simvastatin[tm] scaffolds with 30% porosity were assembled. Surgeries were performed in a private practice and follow-ups were conducted at the university. Tissue healing was evaluated clinically before tooth extraction and on follow-ups at 1 week (suture removal), 1 month, 3 months, 6 months and 8 months. Patients were asked to assess their pain during the 8-month follow-up period. Radiographic evaluation was performed using cone-beam CT (CBCT) after 4 months in some patients and after 6 months postoperatively in others, in order to evaluate bone mineralisation. Results: After 8 months, 47% of cases in a test group showed rejection of biomaterials: 6 (66.7%) of PLGA/HA; 2 (25%) of PLGA/HA plus Simvastatin. All cases with BioOss Collagen (n = 3) showed no rejection. Mean graft rejection time was 45.6 days ± 36.7. Patients experienced pain in three out of the total eight rejection sites (37.5%) and infection was present in only one of these three. CBCT scanning revealed encapsulation of all the tested materials, but in the other groups normal bone formation was seen. No systemic problems were observed in patients treated with materials in the test groups. Conclusion: Application of BioOss Collagen resulted in fewer changes of the alveolar ridge compared to the negative control and test groups, four and six months after extraction. The use of Simvastatin led to no systemic problems. More studies with a larger sample numbers are now needed, and these should include PLGA/HA scaffolds with greater porosity. -
ASSESSMENT OF REGIONAL HAEMODYNAMICS OF THE ALVEOLAR BONE IN PATIENTS WITH CHRONIC GENERALISED PERIODONTITIS
Objectives: The objective of our study was to develop a method of assessing the functional state of vessels of the jaw bone in patients with periodontal disease. Methods: We examined 77 patients with chronic periodontitis. Clinical assessment was made of the state of periodontal tissues in patients (hygienic index, depth of periodontal pockets, tooth mobility) and radiographic studies (to determine the degree of bone resorption), and regional blood flow of the periodontal tissues by the method of reproductory. We selected 25 patients with chronic periodontitis and 25 with intact periodontium for the control group. Reproductory were conducted using computerised software developed by Diatom and electrode systems. Due to the configuration and number of electrodes in the designed system, the procedure was more comfortable for both investigators and researchers. As a result, we managed to achieve stable fixation of the electrode system within the patient’s oral cavity, which was not possible in previous studies. As a consequence, repeatable results and a standardised methodology were achieved. Results: Patients with intact periodontium of the RIshowed 0.31±0.16 blood saturation. Peripheral vascular tone reflecting the temporal relation of systolic and diastolic waves was 18.74 ± 0.2; resistance to the flow of blood in the regional blood vessels (IPS) was 136.96± 5,6; IEwas equal 76.19 ± 4.2. Similar studies on patients with chronic generalised periodontitis, for comparison with data obtained with standard values, showed lower RI values of 64.5% and 0.11% ± 0.4. PTS gave higher values of 19.4 ± 0.25, which exceeds the same indicator in intact periodontium (3.4%). The value of peripheral resistance was slightly lower (by 3.8%) and amounted to 131.72. The elasticity of blood vessels of patients with periodontitis was lower than that in intact periodontium by a factor of 4 and amounted to RUR of 18.43 ± 0.27. Conclusion: Thus, in result of conducted research we can conclude about the functional changes in regional haemodynamics of the alveolar bone in patients with chronic generalised periodontitis, which consists in reducing the elasticity of the vascular walls, and increased peripheral vascular tone. Marked changes are confirmed by the phenomenon of reducing blood vessels.

Take this survey to help us improve your experience
on Dental Campus
For completion, you get 3 days unlimited access to:
- All lectures
- All cases
- All videos