







-


COMPARATIVE EVALUATION OF SIMULTANEOUS MAXILLARY SINUS FLOOR ELEVATION AND IMPLANT PLACEMENT WITH AUTOGENOUS BONE VERSUS A BOVINE-DERIVED XENOGRAFT—A 6-YEAR RETROSPECTIVE STUDY
Objectives: The long-term outcome after simultaneous maxillary sinus floor elevation and implant placement with autogenous bone or bovine xenograft was explored. Methods: Simultaneous maxillary sinus floor elevation and implant placement with autogenous bone or bovine xenograft (BioOss) was assessed in 45 patients with vertical maxilla dimension ofless than6mm. Sinus augmentation was performed using mandibular bone grafts or BioOss. In the autogenous bone group, 56 implants were placed in 21 patients, while in the BioOss group, 24 patients received 62 implants. After 72 months of functional loading, implant survival and reduction in augmentation height were compared between the groups.Fisher's exact test and equivalence testing were used to compare implant survival rates. Results: An overall survival rate of 95.7% was found for implants 6 years after insertion. In the autogenous bone group, the implant survival rate was 96.4%, while in the BioOss group, it was 95.2%. The difference was not statistically significant (p > 0.05); both treatments were equivalent (confidence interval 90%) for the equivalence interval (–0.1; 0.1), and 46.3% of cases showed no reduction in the augmentation height at 6 years follow-up, when augmentation was performed with autogenous bone; in the BioOss group, no resorption was found in 50.8% of the augmented areas. A reduction in augmentation height of up to 25% was found in 44.4% in the autogenous group, and of 42.4% in the BioOss group. In 9.3% of all cases in the autogenous bone group and in 6.8% in the BioOss[tm] group, up to 50% of the augmented height was resorbed. Conclusion: After a 6-year evaluation period, the use of BioOss for the maxillary sinus augmentation seems to be equivalent to autogenous bone grafting. -
MICRO-TOMOGRAPHIC EVALUATION OF BONE MARROW MESENCHYMAL STEM CELLS AND BONE MARROW CONCENTRATE IN PERIODONTAL REGENERATION
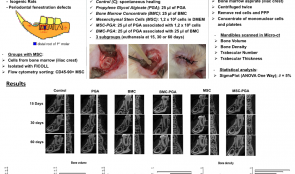
Objectives: The study aimed to evaluate bone formation in periodontal fenestration defects in rats, using bone marrow mesenchymal stem cells (MSCs) or bone marrow concentrate (BMC) with propylene glycol alginate (PGA) as a vehicle. Methods: Periodontal fenestration defects (2mm high x 4mm wide x 1mm deep) were created in the mandible of isogenic rats. The animals were allocated into six groups and further divided into three subgroups for euthanasia at 15, 30 or 60 days postoperatively (n=6 in each subgroup). The control group (C group) was the spontaneous healing group. The PGA group received 25 µl of PGA as vehicle. For the MSC group, stem cells were collected from the iliac crest of two isogenic rats, isolated with Ficoll and cultured in flasks and separated by flow cytometry to obtain a CD45-90+ cell population. In the MSC group, a pellet containing 1.2 x 106 cells was applied to each defect. In the MSC-PGA group, 25 µl of PGA was added to the same pellet. In the BMC groups (BMC and BMC-PGA), 1 mL of bone marrow from iliac crest was aspirated immediately before surgery and was centrifuged twice to remove red cells and poor platelet plasma, producing a concentrate of MSCs and platelets. The BMC and BMC-PGA groups received 25 µl of BMC, but in the latter it was mixed with 25 µl PGA. After euthanasia, mandibles were fixed and scanned by computer microtomography. Bone volume, density and trabecular number and thickness were analysed by SigmaPlot™. The normality of the data was checked and one-way ANOVA used with a significance level of 5%. Results: Bone volume was increased in all groups and at all-time points (p 0.05), except the PGA group which was lower (p 0.05). At 30 days, trabecular thicknesses for MSC and MSC-PGA were similar (p > 0.05) and both were higher than the other groups (p Conclusion: Overall, the stem cells in the proper vehicle resulted in faster and more extensive bone regeneration in periodontal fenestration in rats. MSC alone and BMC in the vehicle were also associated with better bone regeneration than spontaneous healing or vehicle alone. -

MOLECULAR DISCRIMINATION AND ANGIOGENESIS PROPERTIES OF HUMAN OSTEOBLASTS FROM DIFFERENT BONE ENTITIES
Objectives: Autologous grafts from the iliac crest remain the gold standard for alveolar ridge reconstruction. This study aimed to compare the osteogenic potential of human osteoblasts from alveolar and iliac crest bone. Methods: We compared primary human alveolar osteoblasts (aHOBs) and human iliac osteoblasts (iHOBs) derived from patients undergoing routine intraoral bone grafting. Their proliferation potential was evaluated using real-time impedance monitoring. The relative gene expression of bone-specific biomarkers was determined by quantitative polymerase chain reaction (qPCR). Immunohistochemistry, phase-contrast microscopy, alkaline phosphatase (ALP) assay and alizarin red staining were used to visualise cell morphology and mineralisation capacity. In a second part of the experiment, the angiogenesis potential of OPN (osteopontin) derived from aHOBs and iHOBs was investigated using human umbilical vein endothelial cells (HUVECs) in terms of migration and tube formation. Results: The proliferation rate of aHOBs was nearly twice as fast as that of iHOBs (130 hours versus 80 hours). ALP activity and alizarin staining in both aHOBs and iHOBs indicated similar mineralisation capacities. Expression of seven genes (BMP-1, CSF-1, TGF-BR1, ICAM-1, VCAM-1, OPN and DLX-5) was significantly higher in iHOBs than aHOBs. In line with its gene expression, secretion of OPN was greater in iHOB supernatant than aHOB supernatant. OPN was found to stimulate migration of HUVECs (but not tube formation), confirming its role in angiogenesis. Conclusion: These data suggest that osteoblasts derived from iliac crest have higher osteogenic potential than primary osteoblasts from alveolar bone. This may enhance our understanding of the molecular impact of bone cells from different bone sources on bone regeneration in alveolar ridge reconstruction.Secreted OPN was found to have a role in angiogenesis by stimulating migration of HUVECs. -

RECONSTRUCTION OF 3-D ALVEOLAR DEFECTS BY USING A CUSTOMISED MESH (YXOSS CBR) IN 100 CASES
Objectives: Missing or reduced buccal bone plates, as well as a reduced vertical dimension, still represent challenges in bone augmentation and require 3-D reconstruction. Modern individualised dentistry intends to provide new therapeutic concepts based on computer aided CAD-CAM technology and 3-D printing. The aim of this study was to establish a protocol for the clinical application of a patient-specific titanium mesh (Yxoss CBR9) for customised bone regeneration. Methods: One hundred patients were treated by this technique during a two-year period. A 3-D projection of the bony defect was generated and an individualised titanium mesh was designed using CAD-CAM procedures and rapid prototyping. The meshes were installed using a mixture of autogenous bone graft harvested from various intraoral donor sites and Bio Oss[TM] particles in a ratio of 1:1. Implant placement was simultaneous with mesh insertion, or after a healing period of six months combined with removal of the mesh. Evaluation of mesh size, defect region, augmentation site, healing difficulties and soft tissue management was performed. Results: This technology was able to reproduce the alveolar defect properly and produce adequate dimensional accuracy. In all cases, the mesh was placed easily as designed and 3-D bone augmentation was achieved in a predictable way. No serious complications were seen during the healing period and exposure of the mesh did not lead to augmentation loss. Proper soft tissue management and additional use of BioGide[tm] showed a significantly improved outcome. Implant placement was not possible in two cases due to patient non-compliance. Mesh removal was facilitated and caused no bone loss. Histological analysis revealed well-organised, newly formed bone. Conclusion: This protocol using a customised mesh (Yxoss CBR facilitated and shortened surgery time and improved the quality of rehabilitation processes in bony defects. Augmentation volume was predictable and surgery was less invasive. -
A LONG-TERM RETROSPECTIVE ANALYSIS OF OSTEOTOME SINUS ELEVATION AND SIMULTANEOUS IMPLANT PLACEMENT
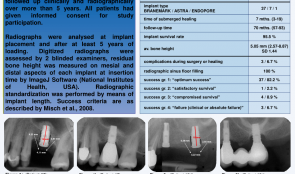
Objectives: Twenty years after Summers’ first description of the transalveolar osteotome technique in the posterior maxilla, this procedure is the standard method for sinus floor elevation. Minimal post-operative morbidity, reduced treatment time and lower patient expenses are some of the advantages over the more invasive lateral window approach. The aim of this study was to retrospectively evaluate screw-type implants with simultaneous sinus augmentation placed between 2002 and 2008. Methods: Screw-type implants (n = 45) were placed in molar sites with reduced bone height using the osteotome technique with simultaneous augmentation and deproteinised bovine bone mineral (DBBMc). After a minimum healing time of 12 weeks, implants were loaded with single cemented (porcelain-fused-to-metal) crowns. All patients were followed up clinically and radiographically for more than 5 years. Results: Of the 45 implants, 3 (6.6%) were lost and 37 (82.2%) were in “optimum functional and aesthetic condition”. All implant sites with functioning fixtures showed complete radiographic opacity in the formerly augmented sinus areas. Bone height increased significantly (p Conclusion: Transalveolar sinus floor elevation using graft material leads to successful functional and aesthetic long-term outcomes. -
COMPARISON OF DIFFERENT BONE SUBSTITUTES BASED ON A LITERATURE REVIEW
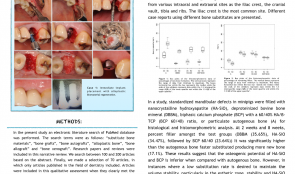
Objectives: Many procedures require the use of bone grafts to replace or recover the volume of bone that has been resorbed. Many configurations of dental implants exist, along with bone autografts, bone allograft, alloplastic bone substitutes and bone xenograft, to recreate physiological occlusion, and aesthetic and masticatory function. We aimed to investigate whether autogenous bone is still the gold standard for treating patients. Methods: We performed an electronic literature search of the PubMed[tm] database using search terms “substitute bone materials”, “bone grafts”, “bone autografts”, “alloplastic bone”, “bone allograft” and “bone xenograft”. We identified between 100 and 200 research papers and reviews, from which the abstract was read to select 70 (excluding all those that did were not dentistry-related). Qualitative assessment was performed on publications that clearly met the following inclusion criteria: recent papers, published in the last 8 years, related to the terms listed above. Results: The individual healing profile of a given bone substitute with respect to osteogenic potential and substitution rate must be considered when selecting adjunctive grafting materials for bone regeneration procedures. Bone replacement materials could be classified into xenografts, or. substances or other natural hydroxyapatite and biocompatible substances. Allograft materials belong to the same species, but do not contain living cells. Alloplastic materials are synthetic materials used instead of real bone. Autograft bone can be obtained from various intraoral and extraoral sites, such as iliac crest, cranial vault, and tibia of the patient. Different case reports reported the use of different bone substitutes. In one study, standardised mandibular defects in mini-pigs were filled with nanocrystalline hydroxyapatite (HA-SiO), deproteinised bovine bone mineral (DBBM), biphasic calcium phosphate (BCP) with a 60/40% HA/β-TCP (tricalcium phosphate) (BCP 60/40) ratio, or particulate autogenous bone for histological and histomorphometric analysis. At 2 and 8 weeks, the percentages of fillers in the test groups were DBBM 35.65%, HA-SiO 34.47%, and BCP 60/40 23.64%. It was significantly higher than autogenous bone and was substituted more quickly, producing more new bone (17.1% ). These findings suggest that the osteogenic potential of HA-SiO and BCP is inferior to that of autogenous bone. However, if a low substitution rate is desired to stabilise volume, as in the aesthetic zone, then HA-SiO and DBBM may be preferable. Conclusion: Despite the increasing number of available bone substitutes in the last years, bone autografts remain the gold standard. They are osteogenic, osteoinductive and osteoconductive, and the newer ones have a regulatory action. -
DEGREE OF SATISFACTION WITH CHEWING ABILITY IN PATIENTS REHABILITATED WITH IMPLANT-SUPPORTED RECONSTRUCTIONS
Objectives: The aim of this study was to assess the degree of satisfaction of chewing ability among patients treated with fixed partial dentures and/or single crowns supported on dental implants. Methods: The Dental Impact of Daily Living (DIDL) questionnaire was used, which has a dimension for chewing ability, together with a Visual Analog Scale (VAS) for satisfaction values. Interviews were conducted on a total of 183 patients (71 men and 112 women) with a prosthesis in situ for at least one year, placed between 1998 and 2012 at the University of São Paulo. Forty patients had fixed total prostheses and 143 patients had partial dentures and/or single crowns supported on dental implants. To test the association between variables was used Pearson’s chi-squared test. Results: Of those interviewed, 73.2% of patients (52 men) were satisfied with their ability to chew and 85% (34 with total prostheses) reported satisfaction, however there were no statistically significant differences between them and patients treated with partial dentures and/or single crowns and women. Conclusion: The degree of chewing satisfaction of patients treated with total prostheses and men treated with implants was high, mainly because of the stability and comfort of the prosthesis, followed by aesthetics and hygiene. Accurate articulation and aesthetic requirements seem to be not as important for men as they are for women which shows in terms of levels of satisfaction, but the findings are not conclusive. -
MORPHOMETRIC ANALYSIS OF TRICALCIUM PHOSPHATE (TCP) SCAFFOLDS IN VIVO
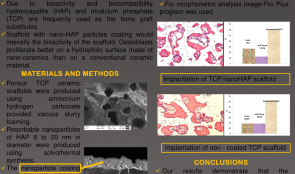
Objectives: Trauma and bone pathologies in the maxillofacial region frequently require bone replacement with biomaterials. Due to bioactivity and biocompatibility, hydroxyapatite (HAP) and tricalcium phosphate (TCP) are frequently used as graft substitutes. This study used scaffold with a coating of nano-HAP particles, which intensifies the bioactivity of the scaffold because osteoblasts proliferate better on hydrophilic nano-ceramic surfaces than on conventional ceramic ones. Methods: Porous TCP ceramic scaffolds were produced using ammonium hydrogen carbonate. Resorbable nanoparticles of HAP 8 of 20-nm diameter were produced by solvothermal synthesis, and coated onto the external and internal surfaces of the scaffolds using ultrasonic energy, which ensures strong adhesion of the nanoparticles. New Zealand rabbits (n = 10) were used for in vivo testing. Uncoated and coated TCP ceramic scaffolds were implanted in the lower jaw. Surgically created defects were filled with scaffolds (diameter 5mm, height 3mm). After three months, explanted samples were evaluated for scaffold resorption and bone regeneration. Histology samples were stained with haematoxylin and eosin and evaluated with Leica BME microscopy. Morphometric analysis was conducted using Image-Pro Plus[tm]. Results: Intraosseous implantation of the TCP ceramic scaffold with and without nano-HAP coating initiated new bone formation in all cases. We observed many osteoblasts near the implanted materials as well as rare osteoclasts. Partial destruction of the biomaterial was seen in bone samples. In the uncoated samples, 62.64% of biomaterial remained, with 18.99% newly formed bone and 18.59% soft tissue. In the coated scaffolds, 60.74% of biomaterial remained, with 26.70% newly formed bone and 12.56% soft tissue . Conclusion: The introduction of nano-HAP coating by ultrasonic coating technology can improve the bioactivity of TCP ceramic scaffolds with an increase in new bone formation and have potential for use in maxillofacial surgery. -

IS RIDGE PRESERVATION SAFE OR NOT IN INFECTED SOCKETS? A RETROSPECTIVE DATA ANALYSIS
Objectives: To date, most previous work evaluating healing after tooth extraction has included only fresh extraction sockets. In normal clinic practise, however, the indications for extractions are more complex and certain pathologies are associated with destruction of the socket walls, often resulting in severe resorption. The aim of this study was to evaluate the safety of ridge preservation in infected sockets. Methods: A total of 320 dental records from Seoul National University Dental Hospital archives (January 2011–November 2015) including patients who received extraction due to infection and immediate ridge preservation in the Department of Periodontics were evaluated. the exclusion criteria were as follows: i) ridge preservation in fresh sockets which were extracted due to caries and fracture (excluding retained roots); ii) ridge preservation performed with non-resorbable membrane; iii) age less than 20 years; iv) repetitive medication administration with anti-inflammatory drugs (excluding rheumatoid disease); iv) current pregnancy; and v) history of autoimmune disease. Records were reviewed to identify cases where infection was present (endodontic origin, periodontal origin, and combined endodontic–periodontal origin), which was removed by meticulous debridement and immediately grafted with a biomaterial. The following data were retrieved from the hospital database records: pathologic origin, success and failure rates of the attempted ridge procedure technique, and preservation in infected sockets. Results: A total of 320 ridge preservation surgeries were performed and 13 cases not meeting the inclusion criteria were excluded. Of the 307 eligible subjects, 9 cases (2.93%) were classified as endodontic origin, 198 (64.50%) as periodontal, 90 (29.31%) as combined endodontic-periodontal and 10 (3.26%) unknown. Uneventful healing was observed in 299 sites (97.39%) with no additional medication, whereas six sites (1.95%) needed additional medication (5 days of additional antibiotics) due to inflammatory symptoms. Re-infection occurred in two sites and the biomaterials within the socket were removed. Clinical symptoms included abscess with pus formation, caustic odour, pain and severe bleeding. The cause for failure in site 1 may be attributed to overfilling of the biomaterial attracting new infection source and complicating the closure of the wound. In site2, necrotic bone plate and/or retained root-like radiopacity observed in the CT, suggesting incomplete removal of the infection source within the socket. Besides these two cases of infection, ridge preservation was successful in 305 sites, yielding a high success rate of 99.35%. Conclusion: Within the limitation of this study, our observations suggest that immediate ridge preservation with various biomaterials is a safe procedure, despite the need to graft immediately following tooth extraction and to remove the infection source using the conventional debridement method. Caution is needed when performing debridement so as not to leave root fragments or necrotic bone plates unremoved. Also, overfilling may compromise wound stability at the entrance of the socket and must be avoided for optimum results. -

THROUGH-ROOT IMPLANT SITE PREPARATION FOR ATRAUMATIC EXTRACTION OF ANKYLOSED TEETH IN IMMEDIATE IMPLANT PLACEMENT
Objectives: Immediate implant placement after tooth extraction is widely covered in the dental literature and positive outcomes have been well reviewed and documented, demonstrating that it is a beneficial and predictable procedure for replacing hopeless teeth. The aim of this study was to report two cases of ankylosed teeth extracted with the alternative approach and treated with immediately placed implants. Methods: Two patients presented with ankylosed hopeless teeth, and treated with immediate implant insertion was planned. After local anaesthesia (4% articaine hydrochloride with 1:100 000 adrenaline hydrochloride) without any incision or flap preparation, the first pointer drill was placed into the root canal to thin the root walls without reaching the apex of the tooth. The second pilot drill was placed into the root canal to further thin the walls without passing through the apex. The third drill (using the same pilot drill but with a sterile implant preparation kit) was placed in the root canal, passed through the apex and split the root into parts. Subsequent drills were used to prepare the implant site in the bone passing through the root canal. After mobility of the root fragments was obtained, they were gently separated from alveolar bone using periotomes and removed from the socket with pincettes. The extraction socket was thoroughly curetted before implant insertion. After installation in a palatal position (in avoid traumatising the labial plate of the socket), the buccal gap between the socket wall and the implant was filled with bone grafting material (Bioteck) and a healing screw was installed. The site was sutured to protect the fresh extraction socket and the biomaterial. Results: In both cases it was possible to maintain the integrity of the surrounding bone and obtain primary stability of the implants, and the soft and hard tissue healing processes were uneventful. No peri-implant bone defects were detected by probing around the implants. Radiographic examination of all implants after one year showed no radiotransparency around implants. Our protocol used different drills and a sterile kit during bone preparation to avoid infection by root canal bacteria. Conclusion: Within the limits of a case series, this protocol for extracting and replacing ankylosed teeth with immediate implants seem to be successful. The finding needs to be confirmed by other more statistically reliable studies as randomised controlled trials. Further studies are also needed to confirm the clinical and microbiological advantages of the use of sterile drills at every step.

Take this survey to help us improve your experience
on Dental Campus
For completion, you get 3 days unlimited access to:
- All lectures
- All cases
- All videos