







-


HOW DEEP DOES SUBGINGIVAL IMPLANT SURFACE AIR-POLISHING REACH AND WHAT INFLUENCES CLEANING EFFICIENCY? AN IN VITRO STUDY ON TITANIUM DISCS
Objectives: Recent studies show that air-polishing is an effective method for maintaining implants and treating peri-implant mucositis and peri-implantitis. However, none of the studies investigated how the method works, in terms of the shape and size of the cleaning area around the nozzle, the influence of different settings and depth of pockets. This study aimed to identify the most effective technique by examining the most important parameters. Methods: Forty-eight titanium SLA surface discs were coated with calcium phosphate (CaP) to simulate visually identifiable plaque and were inserted in subgingival models. All applications were done using an EMS Air-Flow[tm] master with a plastic Perio-Flow[tm] nozzle, on Perio Mode and using EMS Air-Flow[tm] Plus Powder. In the first part of the experiment, discs were treated with the EMS airflow device for 5 seconds in a static state using different air and water settings, nozzle depths and chambers with different powder flows. The most effective settings, established from these results, were used for the second part of the experiment, but the nozzle was moved in three different ways. In both parts, powder consumption, water consumption and total cleaned area were calculated. In the first part, the analysis was carried out using a multifactorial (25 factors) statistical design (ANOVA). The assumption was checked graphically with a Q-Q plot and tested with Levene’s test. Only factors with p Results: The average powder consumption for a standard chamber (EMS Air-Flow[tm] Perio Plus Chamber) with low-pressure settings was 0.05 gr and 0.13 gr with high pressure. The factors that significantly influenced cleaning efficiency were air pressure, powder flow, the combination of air pressure and powder flow, the combination of air pressure and nozzle depth, and the combination of the water volume and powder flow. Factors were considered relevant with a p2) of the model statistical model was 85.63%, meaning that 85% of the results could be explained by these factors. The air pressure had a major effect. The total cleaned surface area was greater in all higher-pressure groups. The cleaning effect was spread around the nozzle, whereby the size of the cleaned area exceeded the nozzle’s physical borders both horizontally and vertically. The mean distance between the right edge to the left edge of the cleaned area was 6.53mm at high pressure and 4.35mm at low pressure. The cleaning effect reached an average of 2.8mm beyond the nozzle exit (i.e. the nozzle cleaned vertically deeper than its own size). There were no significant difference between the three nozzle movements, but cleaning efficiency decreased significantly if there was no movement or powder, while the presence of powder and any type of movement had a big impact on cleaning efficiency. Conclusion: The study unravelled how air-polishing works on implant surface, thus cleaning efficiency can be improved by paying attention to the factors outlined here, the most important of which is air pressure. The more pressure applied, the better the cleaning effect. Inserting the nozzle into deeper pockets enhances the effect, and moving the nozzle is crucial. Clinicians should use high-pressure settings, preferably in deep pockets, with nozzle movement. Certain areas were only cleaned superficially after 5 seconds, therefore we recommended applying airflow twice for 5 seconds per site for deeper cleaning of implant surfaces. Another important finding is that cleaning extends beyond the nozzle end, confirming that it is better at reaching deeper areas than hand devices. -
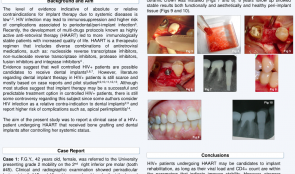
BONE AUGMENTATION IN HIV-POSITIVE PATIENTS ON HIGHLY ACTIVE ANTI-RETROVIRAL THERAPY—CASE REPORTS AND REVIEW OF THE LITERATURE
Objectives: The aim of the study was to report two clinical cases of HIV-positive patients on highly active anti-retroviral therapy (HAART) who received implant-supported rehabilitation after bone reconstruction procedures and were followed for up to 10 years. Methods: Case 1 was a 44-year-old women who was referred to treatment because of persistent symptomatic apical periodontitis in elements #30 and #29. During exploratory endodontic surgery, in an attempt to retain her teeth, a longitudinal fracture and extensive bone dehiscence were detected in #29 and replacement by dental implant was planned. Viral load was undetectable and CD4/CD8 counts were compatible with an immunocompetent condition. In a second event, tooth #29 was extracted and the large bone defect filled with a mixture of autogenous bone plus bovine hydroxyapatite. A collagen membrane was used as a barrier. The implant was placed, and after the osseointegration period a metal–ceramic crown was installed. The 10-year follow-up appointment and control x-rays showed healthy and stable peri-implant tissues. Case 2 was a 47-year-old man who was referred for replacement of an upper molar with severe bone loss and close relation with the pneumatised sinus. He had been on HAART for approximately 8 years. Viral load was undetectable and the patient was considered able the receive the intervention. The tooth was extracted and socket preservation techniques were used (bone substitute plus collagen membrane). After healing, a sinus lift procedure was performed with the lateral window technique, using bovine hydroxyapatite and collagen membrane. The implant was placed at the same time. The patient healed uneventfully and has been followed for 8 years with good results. Results: Both HIV-positive patients undergoing HAART had undetectable viral loads and white cell counts (CD4/CD8) within a range that is compatible with dental interventions. Both received antibiotic cover with amoxicillin 500mg and clavulanic acid 125mg three times daily for one week to prevent postoperative infection. They were prescribed ibuprofen 600mg three times daily to control postoperative discomfort. Both patients were followed by an assistant physician who allowed them to undergo the planned dental intervention. All the interventions healed uneventfully and both patients were able to receive the prosthesis within the planned treatment period. At biannual follow-up in a periodontal maintenance program, implants were functional, without clinical or radiographic signs of peri-implantitis or mucositis. The patients maintained satisfying levels of oral hygiene and did reported no significant systemic alterations. Both had undetectable viral loads and good CD4/CD8 counts. Conclusion: HIV-positive patients undergoing HAART are usually able to maintain good systemic conditions and therefore may be eligible to receive implant-supported restorations. In both cases presented, follow-up showed stable and healthy peri-implant tissues and functional implants. Literature on this topic is still restricted to few studies with small samples, but previously published data suggest that well-controlled HIV-positive patients can benefit from dental implants, even when bone augmentation procedures are needed. The need for antibiotic coverage is still controversial. -

DEVELOPMENT OF A HELICOIDAL CT-BASED COMPUTER TOOL TO ESTIMATE BONE DENSITY AROUND DENTAL IMPLANTS
Objectives: The study analysed dental images from DICOM (digital imaging and communications in medicine) formats in order to establish the volume of a cylindrical corona around and along the implants, to calculate statistical values of bone density for each slice of the corona (and for total volume), and to determine a global value based on a mathematical formula that determines a unique density value. Methods: The study included 71 patients from three private clinics, each of whom underwent helicoidal CT, to obtain dental images in DICOM format. A total of 162 dental implants were planned using a digital dental implant diagnosis tool to create files in a specific format. These were analysed using a Nobel Clinician Viewer[tm] program. Results: This computer tool was developed as a plug-in of the open sourced ImageJ framework. The inputs are dental DICOM images from helicoidal CT, and parameters that characterise each implant from Nobel Clinician planifications are location, length, diameter and angle. The tool provides an interface for selecting the location of each implant, and the value of the radius of the surrounding cylindrical corona, from which density will be calculated. It also allows import and export of implant data to and from an external database. Once a 3-D image is presented to the tool and parameters are settled, the tool proceeds to automatically calculate the volume surrounding the implant and its density. The selected volume can be visualised in the plug-in for inspection prior to statistics export. Several statistics are gathered from the voxels in the cylindrical corona, including whole volume mean, standard deviation, Shannon entropy, skewness and kurtosis; these can be much more informative if retrieved per slice. Finally, a mathematical formula of bone density has been developed. Conclusion: The tool presented here allows automatic calculation of density of the bone surrounding dental implants. In the future we plan to use data-mining techniques on the clinical data of these 71 patients to establish predictive models of implant stability and subsequent success rates of dental implants. -

DIGITAL IMPLANT PLANNING WITH 3-D PRINTERS AND CBCTS IN GUIDED SURGERY AND BONE GRAFT PROCEDURES
Objectives: Here we present a new digital implant planning protocol using 3-D printing, cone beam CT (CBCT), scanners and computer-assisted design software. Biomodels and surgical guides are manufactured with 3-D printers and digital planningis used to allow implant placement based on the concept of prosthetically driven implantology. Methods: The digital implant planning protocol with 3-D printers is based on the premise that digital files obtained from CBCTs and scanners can be imported to computer-assisted design (CAD) software and all phases of the treatment can be performed virtually, before implant surgery. First, CBCTs from the areas of interest are obtained. A set of frontal photographs are taken and the teeth are scanned with intra-oral scanners (impressions can be taken and scanned if an intra-oral scanner is not available). The digital CBCT files are converted from DICOM (digital imaging and communications in medicine) to stereolithography (STL) files using open-access software and imported to CAD software. Images are edited using the principles of digital smile design, and a digital wax-up is produced. Digital planning allows all the images to be overlaid (CBCT; scanned teeth plus gingiva; digital wax-up; photos) so that implant positions can be planned with all the references needed with respect to prosthetically driven implantology. When digital planning is finished, polylactic acid biomodels can be printed by 3-D printers, reproducing the area to be operated. Biomodels are particularly useful in cases where large bone defects will be grafted, because the surgeon can plan the bone reconstruction procedure and adapt bone blocks and titanium meshes more easily. Surgical guides are also printed and used to drive the burs during surgery. Three cases are described. Results: The first case was a young patient who had suffered a car accident and lost the upper incisors. Orthodontic treatment was used to obtain an ideal mesiodistal space for implant placement and a fixed bridge supported by two implants. After orthodontics, CBCT showed that bone reconstruction was needed and autologous bone grafts were planned. A biomodel was printed by 3-D printer and used to help adapt the block before elevating the flap in the area receiving the graft. After 4 months, another CBCT was obtained and the implant position was digitally planned based on the virtual wax-up. Implants were successfully placed and a fixed bridge with ceramic gingiva was built. The second case was an elderly patient who needed implant surgery for placement of two implants to support a fixed bridge. The patient already had implants on the posterior mandible and on the right central incisor. After digital wax-up and CBCT evaluation, two implants were placed and the bridge was successfully built. The third case was another young patient who needed orthodontics before surgery for single implant placement. Every step of the planning protocol was followed and the implant was placed in the predetermined position. All cases healed uneventfully and were followed up for two years or more. Conclusion: The digital implant planning protocol appears to be a feasible and affordable treatment for oral rehabilitation. It allows surgeons and restorative dentists to preview the desired results and study cases in a very detailed manner, by overlaying different images providing precise information about the relation between the teeth, gums, bone and face. The software is open-source and the 3-D printers are low-cost and use affordable polymer feedstock, so this protocol is a useful tool with an excellent cost–benefit ratio. To the best of our knowledge, we are the first to use low-cost domestic 3-D printers to manufacture biomodels and surgical guides. Case–control multicentre studies will be useful for validating the protocol and comparing the accuracy of less expensive polymer-based 3-D printers with larger, expensive industrial printers. -
RIDGE PRESERVATION OF MAXILLARY THIRD MOLAR POST-EXTRACTION SOCKETS USING A NOVEL PLGA/HA SCAFFOLD, WITH AND WITHOUT SIMVASTATIN—AN 8-MONTH CLINICAL FOLLOW-UP OF A HUMAN SPLIT-MOUTH RANDOMISED CONTROLLED CLINICAL TRIAL
Objectives: This study aimed to evaluate the osteoinductive capacity of Simvastatin[tm] incorporated into a poly(lactide-co-glycolide)/hydroxyapatite (PLGA/HA) scaffold and possible inflammatory reactions associated with its use. For comparing bone formation, a positive control group with xenogeneic bovine bone graft material (BioOss Collagen) and a negative control with no graft were used. This was a split-mouth randomised controlled clinical trial. Methods: This research was conducted in 13 patients requiring bilateral extraction of maxillary third molars at the Federal University of Santa Catarina. After extraction, different biomaterials were placed for regeneration of the extraction zone, with randomly assignment of four treatment modalities: Group 1 (negative control), not filling (clot); group 2 (positive control), BioOss Collagen; group 3 (test), PLGA/HA; group 4 (test), PLGA/HA plus Simvastatin[tm] at a concentration of 2.0%. PLGA/HA and PLGA/HA plus Simvastatin[tm] scaffolds with 30% porosity were assembled. Surgeries were performed in a private practice and follow-ups were conducted at the university. Tissue healing was evaluated clinically before tooth extraction and on follow-ups at 1 week (suture removal), 1 month, 3 months, 6 months and 8 months. Patients were asked to assess their pain during the 8-month follow-up period. Radiographic evaluation was performed using cone-beam CT (CBCT) after 4 months in some patients and after 6 months postoperatively in others, in order to evaluate bone mineralisation. Results: After 8 months, 47% of cases in a test group showed rejection of biomaterials: 6 (66.7%) of PLGA/HA; 2 (25%) of PLGA/HA plus Simvastatin. All cases with BioOss Collagen (n = 3) showed no rejection. Mean graft rejection time was 45.6 days ± 36.7. Patients experienced pain in three out of the total eight rejection sites (37.5%) and infection was present in only one of these three. CBCT scanning revealed encapsulation of all the tested materials, but in the other groups normal bone formation was seen. No systemic problems were observed in patients treated with materials in the test groups. Conclusion: Application of BioOss Collagen resulted in fewer changes of the alveolar ridge compared to the negative control and test groups, four and six months after extraction. The use of Simvastatin led to no systemic problems. More studies with a larger sample numbers are now needed, and these should include PLGA/HA scaffolds with greater porosity. -
ASSESSMENT OF REGIONAL HAEMODYNAMICS OF THE ALVEOLAR BONE IN PATIENTS WITH CHRONIC GENERALISED PERIODONTITIS
Objectives: The objective of our study was to develop a method of assessing the functional state of vessels of the jaw bone in patients with periodontal disease. Methods: We examined 77 patients with chronic periodontitis. Clinical assessment was made of the state of periodontal tissues in patients (hygienic index, depth of periodontal pockets, tooth mobility) and radiographic studies (to determine the degree of bone resorption), and regional blood flow of the periodontal tissues by the method of reproductory. We selected 25 patients with chronic periodontitis and 25 with intact periodontium for the control group. Reproductory were conducted using computerised software developed by Diatom and electrode systems. Due to the configuration and number of electrodes in the designed system, the procedure was more comfortable for both investigators and researchers. As a result, we managed to achieve stable fixation of the electrode system within the patient’s oral cavity, which was not possible in previous studies. As a consequence, repeatable results and a standardised methodology were achieved. Results: Patients with intact periodontium of the RIshowed 0.31±0.16 blood saturation. Peripheral vascular tone reflecting the temporal relation of systolic and diastolic waves was 18.74 ± 0.2; resistance to the flow of blood in the regional blood vessels (IPS) was 136.96± 5,6; IEwas equal 76.19 ± 4.2. Similar studies on patients with chronic generalised periodontitis, for comparison with data obtained with standard values, showed lower RI values of 64.5% and 0.11% ± 0.4. PTS gave higher values of 19.4 ± 0.25, which exceeds the same indicator in intact periodontium (3.4%). The value of peripheral resistance was slightly lower (by 3.8%) and amounted to 131.72. The elasticity of blood vessels of patients with periodontitis was lower than that in intact periodontium by a factor of 4 and amounted to RUR of 18.43 ± 0.27. Conclusion: Thus, in result of conducted research we can conclude about the functional changes in regional haemodynamics of the alveolar bone in patients with chronic generalised periodontitis, which consists in reducing the elasticity of the vascular walls, and increased peripheral vascular tone. Marked changes are confirmed by the phenomenon of reducing blood vessels. -
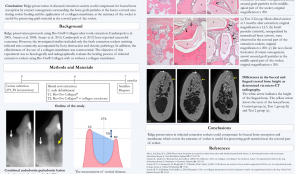
RIDGE PRESERVATION OF EXTRACTION SOCKETS WITH CHRONIC PATHOLOGY USING BIOOSS COLLAGEN WITH OR WITHOUT BIOGIDE—AN EXPERIMENTAL STUDY IN DOGS
Objectives: Ridge preservation protocols using BioOss Collagen after tooth extraction have successful outcomes, but previous studies included only fresh extraction sockets and omitted infected sites with chronic pathology. The effectiveness of collagen membranes is also controversial. The aim of this study was to histologically and radiographically evaluate the healing process of infected extraction sockets using BioOss[tm] Collagen with or without collagen membrane. Methods: Six adult Beagle dogs aged 1–2 years, and approximate weight 10 kg, were used. Sulcular incisions were made, and a flap was elevated in the mandibular premolar area. The left third mandibular premolar and both fourth mandibular premolars were hemisected with fissure burs, and the distal roots were removed atraumatically. A #2 carbide round bur was used to dig a notch in the mesial side of the mesial root, and the notch was filled with a collagen sponge soaked in Porphyromonas gingivalis. The pulp of the mesial roots was removed with a K-file before injection of P. gingivalis and sealed with intermediate restorative materials before suturing the flap. Following communication of the two pathologies (after about 4 months), the mesial roots were extracted and the defects were randomly assigned to one of three subgroups using a 3 x 3 Latin square design. These were no treatment (controls); BioOss Collagen graft (group T1); and BioOss Collagen graft with BioGide collagen membrane (group T2). After 7 months from induction of the lesion (baseline), the dogs were sacrificed and block biopsies were placed in a fixative, dehydrated and embedded. The percentage of different tissues (mineralised bone, bone marrow and biomaterial) in the infected extraction sockets was evaluated, and each extraction site specimen underwent the micro-CT examination. Results: Micro-CT revealed differences in height between the buccal and lingual crests, in addition to the bone morphometric parameters. There were significant differences in the vertical distance between buccal and lingual crests in controls (2.22 mm ± 0.26) and T2 (1.80 mm ± 0.16. Bone surface density (BS/BV) values were 0.32 ± 0.05 (controls), 0.45 ± 0.13 (T1) and 0.50 ± 0.03 (T2). There was a significant difference between BS/BV values in controls and T2. The level of interconnectivity of the bone (TbPf) gave values of –0.53 ± 0.24 (controls), –0.44 ± 0.11 (T1) and –0.32 ± 0.15 (T2). Values for structural model index (SMI) were –5.34 ± 3.07 (controls), –2.94 ± 2.38 (T1) and –1.27 ± 0.83 (T2). TbPf appeared to increase gradually from controls to T1 then T2. The sockets in the control group were occupied by mineralised bone (68.08% ± 6.51) and bone marrow (30.56% ± 6.07%); in T1 they were filled by mineralised bone (55.90% ± 4.70%), bone marrow (23.50% ± 4.19%) and BioOss[tm] particles (18.49% ± 2.11%), and T2 contained mineralised bone (61.38 ± 6.9%), bone marrow (10.31% ± 4.93%) and BioOss[tm] particles (27.04% ± 5.25%). The T2 sockets contained more bone graft material than those in T1. There was a significant difference between amount of mineralised bone in controls and T1. Conclusion: In the micro-CT analysis, the vertical distance between the lingual and buccal crests was significantly shorter in the T2 group (ridge preservation with BioOss Collagen and collagen membrane) compared to controls. This is in line with a previous study that reported similar results using BioOss Collagen for ridge preservation, indicating a possible role of the biomaterial in promoting de novo bone formation to maintain the ridge profile and compensate for marginal ridge resorption. The use of a membrane for ridge preservation (as in T2) to prevent loss of the graft material in the initial healing phase may have improved contact osteogenesis near the coronal part of the buccal bone. Ridge preservation in infected extraction sockets may compensate for buccal bone resorption, and using membrane to cover the entrance of sockets may help preserve graft material near the coronal part of the socket. -
FIRST CLINICAL EXPERIENCES WITH INDIVIDUALISED 3-D AUGMENTATION WITH CAD-CAM DESIGNED TITANIUM MESH ReOss
Objectives: The augmentation of the jaw has been, and continues to be, a sophisticated therapy in implantology, especially when vertical or combined defects have to be restored. Modern computer aided CAD-CAM technologies have led to the revival of old and established augmentation techniques, such as the use of titanium mesh for onlays and guided bone regeneration techniques. ReOss[tm] provides an individualised CAD-CAM-based titanium mesh based on CT, DVT or DICOM (digital imaging and communications in medicine) patient data. Methods: The augmentation possibilities with this new system were evaluated in a small clinical trial of patients (n = 15) with seventeen different defect regions. DVT-based DICOM (digital imaging and communications in medicine) data of patients who needed horizontal, vertical or combined augmentation were used to create an individualised titanium mesh. For the augmentation, a mixture was prepared of autologous bone mostly harvested from the lower jaw and BioOss[tm] particles (1:1) was used. All defects were covered with BioGide[tm] in combination with platelet-rich fibrin (PRF) membranes. All patients received antibiotic therapy for five days. After 6 months, re-entry was performed, with explantation of the titanium mesh and simultaneous implantation. Results: The patients (27% men and 73% women; average age 34 (range 18–60) years) underwent augmentation in the lower jaw (n = 12) and upper jaw (n = 5). Of these, 47% had a horizontal defect, and the remainder had a vertical or combined defect. Augmentation was performed to replace two to seven teeth (an average of three). In all cases, the tailormade titanium mesh was easily placed in the planned area of augmentation. Exposure of the mesh during the healing period occurred in 29%. There was no total loss of the augmentation, nor did exposure lead to situations in which planned implantation could no longer be carried out. All cases showed sufficient augmentation volume that was congruent with the preoperative planned augmented volume. Conclusion: Individualised ReOss[tm] CAD-CAM titanium mesh provides a sufficient onlay and guided bone regeneration technique for augmentation of jaws. The soft tissue covering remains one of the most critical steps in this procedure, and quick and easy application is a great advantage even in vertical defects. -
IMMEDIATE LOADING OF THE MAXILLA USING FLAPLESS SURGERY TO INSERT ONE-PIECE ZIRCONIA IMPLANTS IN PREDETERMINED POSITIONS
Objectives:In the aesthetic area, immediate implant placements are increasingly common. Using a 3-D custom-made guide for insertion is associated with less trauma and faster healing periods. Titanium implants may cause unfavourable soft tissue conditions or recession of gingiva in the area, and lead to compromised aesthetic outcomes. In this study, zirconia implants were chosen rather than titanium.. Methods:A 18-year-old woman, who had previously suffered serious trauma of frontal maxilla, was referred to our dental practice. Due to external root resorption, the central incisors were removed 15 months previously, and she had a fixed orthodontic retainer with two substitute acrylate teeth (#11 and #21) to preserve jaw line functionality and aesthetics. The patient was still adolescent, but thorough examination by cone beam CT established that her jaw development and growth was complete. We decided to insert two zirconia implants, with a comprehensive procedure because the bone loss at both positions was severe. The first step was horizontal augmentation of the alveolar ridge using a membrane technique in order to preserve necessary bone (BioResorb Macro Pore[tm]). Six months later, two zirconia implants (SDS, ATZ, 3.8x11.0mm, torque 35N/cm) were inserted using flapless surgery into predetermined positions using a 3-D custom-made guide. Two connected provisory acrylate crowns were inserted immediately, to stabilise the implants and give the patient functional teeth for the following five-month period. The crowns also aided the process of implant osteointegration, providing an ideal emergence profile and supporting the peri-implant soft tissue. Follow-up was uneventful. Three months after surgery, the final prosthetic restoration comprised of two connected ceramic, metal-free crowns. Results: The healing period was uneventful with no adversary reactions. Both procedures resulted in minimal trauma, due to the use of 3-D custom-made guides for both bone regeneration and implant insertion, which led to a good post-operative period. The first procedure (bone regeneration) gave satisfactory results, and the second (implant placement) gave excellent primary stability without radiographic bone loss or gingiva inflammation. Peri-implant soft tissue parameters showed promising results. Probing depth, clinical attachment level and modified bleeding index at the implant sites were all satisfactory. The restoration work showed a healthy gingival margin and no discoloration of the soft tissue. The most important patient feedback related to permanently improved perception of function, aesthetics, sense, speech and self-esteem (which is very important in adolescents). Conclusion: Use of 3-D custom-made guides for implant placement enables faster and better recovery because trauma is minimised. There is an increasing demand for metal-free implants because of the potential immunologic and aesthetic compromises associated with titanium implants entails. Unfavourable soft tissue conditions or gingival recession may lead to compromised aesthetics, which are particularly concerning when maxillary incisors are involved. Cervical bone loss and gingival recession associated with metal implants tend to cause bluish discoloration of the overlying gingiva, thus impairing aesthetic outcome. Zirconia implants are a good choice for the aesthetic zone. In our case, the gingival margin was healthy and there was no discoloration of the soft tissue. Zirconia implants are also suitable because they have a tooth-like colour, good mechanical properties (high strength, fracture toughness) and good biocompatability. -

ADVANTAGES AND DISADVANTAGES OF COMPUTER-DESIGNED TECHNIQUES FOR ORAL REHABILITATION - A REVIEW
Objectives: In the last four decades, dental implants have become an essential part of oral rehabilitation. Successful implant placement depends directly on highly accurate treatment planning and surgical procedures. It is important to review the accuracy data for surgical and prosthodontical techniques such as guided surgery. Methods: A retrospective review was conducted for cases using an image-guidance system for the accurate placement of implants. An electronic literature search of PubMed database was conducted, combining controlled terms and keywords whenever possible. The search terms were “computer-guided design”, “image-guided surgery”, “computer-assisted manufacture”, “computed tomography” “dental implants” and “surgical guide”. Articles from January 2005 to September 2015 were screened. They were included in a qualitative assessment if they were recent papers and had references to articles related to the terms defined above. Results: Software guides may be useful for decreasing the incidence of implant-associated difficulties, as well as achieving greater precision in placement of implants, leading to better preservation of anatomic structures (especially for full-mouth rehabilitation). The most common difficulties encountered during placement are improper location, wrong angulation, and lack of primary stability. These techniques provide sufficient information about the bone anatomy to avoid these issues and the treatment plan reduces operating time and surgical trauma and increases implant success. However, these techniques require knowledge of and experience in the use of 3-D information for virtual planning and implant positioning, and there is a lack of visibility and tactile control during the procedure, thus vital anatomical structures can be damaged. The available literature on computer-aided surgical guidance has only limited data and relatively short observation periods, therefore further research should focus on clinical studies with long-term follow-up. Conclusion: Surgical implant complications are not uncommon and should be addressed immediately. Causality may be iatrogenic due to poor treatment techniques, and a successful final treatment can be possible by the use of computer-aided surgical guidance. Competent surgeons yield acceptable to excellent results and surgery is predictable using these techniques, but care should be taken when using them.

Take this survey to help us improve your experience
on Dental Campus
For completion, you get 3 days unlimited access to:
- All lectures
- All cases
- All videos