







-


INCREASE OF TRANSVERSE VOLUME USING GUIDED BONE REGENERATION (GBR) WITH ANORGANIC BOVINE BONE MINERAL (ABBM) IN AESTHETIC AREAS AFTER AUTOGENOUS BONE GRAFT—A CASE REPORT
Objectives: Sufficient volume in the anterior region provides good support for the upper lip in implant surgery. Various stages of implant treatment are needed for managing the aesthetic result. Bio-Oss ABBM is mainly integrated in the connective tissue rather than bone and augments soft tissue support for achieving the aesthetic results and protecting the bone graft. Resorbable membranes reduce the rate and severity of complications compared to non-resorbable membranes. This case report focused on the use of ABBM with application of a slow resorbable membrane for implant insertion four months after bone grafting. Methods: A 37-year-old woman, with no medical or surgical history, required aesthetic implant restoration related to previous replacement of a bridge from #12 to #21. Clinical and radiographic examination revealed a big bone defect above the residual teeth. Six weeks after tooth extraction, the bone defect was grafted with bone harvested from the retromolar area using a MicroSaw . Two implants were inserted (XiVe), and a layer of Bio-Oss ABBM was stabilised by application of a Symbios membrane. Four months later, second-stage surgery was performed using palatal connective tissue graft to increase the soft tissue volume. Results: GBR was carried out during the implant insertion, four months after autogenous bone grafting. Preparing the pontic area with provisional restoration followed by definitive restoration after six months produced good soft-tissue stability two years later. Conclusion: The lip and pontic are supported three years after GBR associated with Bio-Oss biomaterial and a slow resorbable membrane (Symbios) during implant insertion. This case suggest that integration of the biomaterial prevents bone volumes changes over time and increases the transverse volume. -

IMPLANT SUPPORTED PORCELAIN-FUSED-TO-METAL (PFM) AND ZIRCONIUM CROWNS IN DIABETIC PATIENTS
Objectives: Investigate the result of implanting titanium root form implants in diabetic patients for replacing periodontal affected teeth by implant supported porcelain-fused-to-metal (PFM) and zirconium crowns to restore function and aesthetic. Methods: 2 patients of diabetic disease participated in this clinical case series: The first patient had adult onset diabetes: type 2 diabetes, Age: 55 years, onset of diagnosis 2007/male. The second patient was young man of type 1 diabetes disease (juvenile diabetes). Age: 30 years / male. Protocol idea of implantation for patient 1:1. 3-sided flap opening, 2. Scaling and cleaning of upper lateral incisors and canines, 3. Extraction of upper central Incisors, 4. Implantation of root form titanium implants (XiVE® by DENTSPLY Implants, Germany) of diameter 3.8 and length 11.5 and 13 mm in teeth sockets at bone level, 5. Augmentation of labial alveolar bone by Algipore® by Dentsply (collagen membrane was not used for this patient), 6. Closure of flap and suturing by 4.0 silk suture. Protocol idea of implantation for patient 1: 1. 3-sided flap, 2. Preparation of bed for XiVE® implant of diameter 3.8 mm and 9.5 mm length in apical part of the socket of the fallen tooth, 3. Coverage of the adjacent labial alveolar bone and upper labial surface of the XiVE® implant by Geistlich bovine bone substitute particles mixed with patient own bone remains of drilling, 4. Coverage of bone substitute particles and adjacent labial bone by collagen membrane of 2 mm * 1 mm, 5. Suturing with 4/0 monofilament suture. Results: Surgical and biologic result for the 1st adult onset diabetic patient.1-A very successful healing of soft tissue around implants platform and roots of adjacent teeth was achieved without complication of flap healing. 2-A very successful osseointegration of Xive s plus surface of porous titanium was achieved with patient alveolar bone. 3-Excellent integration of Algipore material with patient own bone. Prosthetic result. 1-A successful loading of the 2 Xive implants was done by PFM fixed prosthesis since 2012untill now. 2-Diastema was closed. 3-Aesthetic and function of mastication was improved. 4-Psychologic and self-esteem of the academic patient was improved. Surgical and biologic result for the 2nd Juvenile onset Diabetic patient. 1-A successful healing of soft tissue around implant neck without dehiscence of flap. 2-Successful osseointigration of Xive s plus surface of titanium with patient alveolar bone. 3-control of active periodontal disease. Prosthetic result 1-A successful loading of short Xive implant was done by zirconium central incisor on angled abutment since 2013 until now. 2-A solid fixation of MH6 abutment of hexagonal internal design. 3-A stable strong Implant -abutment connection and bone augmented area since 2013 despite crown/implant ratio of about 2:1 4-Aesthetic and function of mastication was restored. 5-Spychologic and self-esteem of patient was improved. Conclusion: The results show that despite diabetic disease type 1 and 2 is considered relative contraindication to dental implant therapy, one can obtain good result by observing 3 major points: 1. Encouraging Diabetic patient and establishing good home oral hygiene measures at least post operatively and later years. 2. Applying adequate medical measures for controlling blood sugar and post-operative infection at implant site. 3. Observing implantation and augmentation protocols carefully. 1. Osseointegration of XiVE® titanium S plus surface could be achieved successfully with diabetic patient jaw bone provided that blood sugar level is reduced to nearly normal level and postoperative soft tissue infection is controlled by antibiotic and home oral hygiene measures. 2. Maintenance of soft tissue support and bone level around artificial PFM and zirconium crowns could be gained for nearly 3 years and more postoperatively in diabetic patient provided good oral hygiene measures were maintained. -
ALVEOLAR RIDGE RECONSTRUCTION USING A SPLIT-CREST TECHNIQUE IN ATROPHIC MAXILLA WITH BIO-OSS AND BIO-GIDE —TWO CASE REPORTS
Objectives: In clinical cases where a severe horizontal bone deficiency is present, it is very difficult to install implants in the perfect position for achieving optimum aesthetics and functional rehabilitation. The split-crest technique leads to reduced waiting times for installation of implants for maxillary defects of less than 3mm. The cases reported here underwent the split-crest technique with interposition of Bio-Oss biomaterial and were reopened for implant placement after five months. Methods: Patients were selected with a horizontal bone deficiency in the maxilla of 1.6–2.3mm. Both were fit for surgery. The preoperative assessment consisted of blood tests, CT scans and antibiotic prophylaxis and full treatment plans were presented to the patients. Infiltrative terminal anesthesia was applied until satisfactory tissue ischaemia was produced. An incision was made above the crystal with 15c blades and mesiodistal relaxing incisions. After total detachment and bone mucoperiostal exposure, a tag 701 was made with a surgical drill at the cortical level, completed with a metal disc osteotomy. A chisel was used between the markings to achieve total displacement of cortical , to achieve sufficient expansion and an intact nasal spine . Screws were placed at the base of each fracture, preventing vestibular cortical blades from moving during bone maturation. Gaps and remaining spaces were filled with Bio-Oss. Bio-Gide membranes were applied, the flap repositioned and the wound was closed by suturing without tension. Results: CT scans four months postoperatively showed increased bone width of approximately 5.2mm. There were no complications and both patients reported little discomfort after surgery. Both underwent further surgery for implant placement after five months. Primary stability of all implants was achieved and manufacturing the prostheses. Conclusion: The split-crest technique is a feasible option. Using Bio-Oss with a Bio-Gide membrane increased the maxillary bone thickness, which facilitated rehabilitation with dental implants. -

IMMEDIATE LOADING WITH ONE-SHOT PROSTHESIS (OSP) AND RECURRENT IMPRESSION (RI) FOR EDENTULOUS PATIENTS TREATMENT—A CASE SERIES
Objectives: Immediate-load protocols for edentulous patients are well-documented treatment options, however it is expensive to fabricate a provisional prosthesis that is capable of loading, which must be followed after osteointegration and soft tissue healing by placement of a definitive restoration that fills gaps that appear between the gingiva and prosthesis. The aim of this study was to carry out the OSP technique using a single prosthesis with a metal framework that permits immediate loading, which could be transformed after complete healing to a definitive prosthesis. Methods: Three patients were treated by the OSP technique. Impressions were taken before surgery, with diagnostic set-up for the final restoration. After surgery, further impressions were made of the implants in position and gingival levels, and the master cast was prepared. Titanium cylinders were screwed onto the abutment replicas, and sections of 3.5-mm diameter titanium rods were laser-welded to them. Passive fit of the framework was checked. The prosthesis was intended to achieve optimum aesthetics and occlusion control. Contacts with the cantilever were avoided to prevent implant stress during osteointegration. After validation, the dentures were placed 24 hours after surgery. Master cast models were preserved on the articulator. After osteointegration, gaps between gingiva and prosthesis were recorded by taking mucostatic RIs of the edentulous areas between implants, with injection of silicone directly under the screwed prostheses. Master models were modified by eliminating the stone between the implants, and transitional silicone prostheses were screwed into place. New plaster was poured into the space to modify the crest profile according to the new anatomy, and resin was applied to improve occlusion of the teeth with the entire prosthesis, including the cantilever. The new prostheses were delivered five hours after making impressions. Results: During the observation period of 12–84 months, implant survival rates were 100%. None of the three prostheses were lost, thus the prosthetic survival rate was also 100%. In all three cases, soft tissue levels and the spaces between the prostheses and tissues were stable. Conclusion: The cost of implant treatment is important to patients. The OSP technique with RIs allows a single prosthesis to be used as temporary prosthesis suitable for immediate loading, that can be transformed, after a short time, to a definitive prosthesis that is adapted to the tissue after complete healing. This leads to cost reductions and increased access of patients. The use of RIs decreases chair time and laboratory time, and re-use of the master cast decreases material costs. Further studies are now required with larger sample sizes to better evaluate this promising low-cost option. -

PHOTOELASTIC ANALYSIS OF OBLIQUE FORCES ON DIFFERENT IMPLANT DIAMETERS
Objectives: The study aimed to review, using photoelastic analysis, the stresses generated on narrow-diameter and regular-diameter implants by simulated masticatory loads, to enable safe use of implants with different diameters. Methods: The photoelastic models were dipped in mineral oil in a polariscope. A digital NIKON COOLPIXTM 4500 camera (with lens 1:2. 6–32mm) was used to visualise the fringes and record digital images. Initial models were obtained from the silicone matrix laboratory, with a space of 10x 40mm (45mm deep) filled with plaster type 4. Photoelastic models were made by drilling the plaster with a high-speed drill and installing the analogues (standardised using a parallelometer). We planned the ideal location of narrow- and regular-diameter implants (2.8mm and 4.0mm, respectively) in the region of maxillary lateral incisors, canines and premolars. Models used in similar positions, were moulded with transfer dyes of aid to open tray. After moulding, the new analogues were screwed into resin. Crowns manufactured from titanium were via CAD-CAM using a Cerec technique were cemented onto the implants to allow better analysis of the stresses around them. Results: Loads of up to 160N were applied obliquely to the titanium laterals of the incisor crowns. Caraga of up to 250 N were placed axially to the crowns of canines and bicuspids. Conclusion: Coherent planning of rehabilitation to reduce toothless regions is important for improving predictability when using implants with reduced diameters, and to enable a lower transfer of force to the structures involved, such as the adjacent bone. It is hoped that these results will enable narrow-diameter implants to be used more safely. Finite element analysis studies do not represent the clinical reality, but all the above must be taken into consideration when planning treatment of edentulous patients. -

WELDING OF PERIODONTAL TISSUE WITH LASER-ACTIVATED INDOCYANINE GREEN (ICG) MEMBRANE
Objectives: Surgical treatment of periodontal disease requires tight closure of the surgical wound, but suturing carries the risks of infection, wound opening and scarring. Chitosan membranes with added indocyanine green (ICG) offer an alternative to suture materials and barrier membranes. The aim of the study was to assess the usefulness of ICG–chitosan membrane for the closure of surgical wounds and as a substitute for membranes for guided tissue regeneration. Methods: In this in vitro experiment, we studied 50 extracted human teeth, 30 samples of porcine gingiva and 10 samples of porcine oral mucosa. We produced chitosan–ICG membranes of 5 x 7mm and welded them with a diode laser to the gingiva, oral mucosa and surface of the tooth roots. Histological analysis was used to identify thermal damage. A rise in temperature on the surface of each sample during welding was determined from temperature profiles recorded with ThermaCAM P45TM thermal camera. The strength of linkages of the ICG membrane with the tissues were measured with a universal tearing machine (Instron 4301TM). We used parametric t-tests, ANOVA and the least significant difference (LSD) post-hoc test to analyse mean maximum temperatures and forces required to rupture linkages in the different tissue types (using s statistical significancelevel of Results: Laser welding of chitosan–ICG membrane to the gingiva, mucosa and root surface was successful and no samples showed significant thermal damage The maximum temperature measured on the root surface during welding was 42.6 ± 9.5° C, which was significantly lower than that for the gums at the already welded membrane on the tooth (55.2 ± 8.0° C) (p = 0.005). Tear forces in three groups of laser-welded gingiva and oral mucosa were 0.14 ± 0.05 N for gingival epithelial welding, 0.06 ± 0.01 N for gingiva welding to connective tissue, and 0.06 ± 0.02 N for oral mucosa welding. Tear forces in four groups of membranes laser-welded to the root surface were 1.41 ± 0.14 N for samples at an angle of 0°, 0.89 ± 0.15 N at 30°, 0.80 ± 0.14 N at 60° and 0.52 ± 0.16 N at 90°. It was 0.85 ± 0.18 N for gingiva welded to the root surface. Conclusion: Within the limits of this study, laser welding of oral mucosa and gingiva can complement the closure of mucosal and periodontal wounds, but cannot replace suturing. The favourable tensile strength of chitosan–ICG membrane linkages with root surface and chitosan’s properties in the membrane is promising as a replacement of non-resorbable membranes. Laser welding of gingiva to the root surface may add further stability to closure of the wound. -
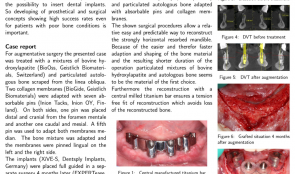
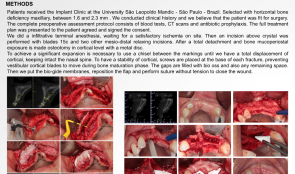
SURGICAL AND PROSTHETIC RESTORATION OF HORIZONTAL RESORBED EDENTULOUS MANDIBLE—A CASE REPORT
Objectives: Few treatment methods are capable of improving quality of life for patients as well, and as predictably, as restoration of edentulous jaw using implant-supported dental replacements. Adequate bone volume is essential for inserting dental implants, so developing prosthetic and surgical approaches with high success rates for patients with bone in poor condition is important reread. This case report focused on surgical and prosthetic restoration of horizontal resorbed edentulous mandible. Methods: The patient was treated with a mixture of bovine hydroxyapatite (Bio-OssTM Biomaterials) and particulate autologous bone, with absorbable pins (Inion Tacks) and collagen membranes (Bio-GideTM). XiVE-SsTM implants were placed under full guidance in a separate surgery four months later (EXPERTeases). For wider support of the central-milled titanium bar (Atlantis-Isuss), the distal implants were inserted at an angel of 30 degrees. A vestibuloplasty was performed using a Mucogarft MatrixTM? And multi-unit abutments (MP-AbutmentssTM were applied to the implants at 0 degrees mesial and 30 degrees distal, to optimise conditions for taking impressions with parallel impression posts. Lohmann’s method was used for the reconstruction. Results: This relative easy and predictable procedure allowed successful reconstruction of strongly horizontal-resorbed mandible, with little loss of the reconstructed bone. Conclusion: We used allogeneic bone blocks, autologous bone blocks and mainly mixtures of bovine hydroxyapatite and particulate autologous bone adapted with absorbable pins and collagen membranes. It was easy and quick to adapt and shape the bone material, resulting in a shorter operation time. Particulated mixtures of bovine hydroxyapatite and autologous bone seem to be the material of the first choice. Use of central-milled titanium bar ensures a tension-free fit of reconstruction which reduces loss of the reconstructed bone. -

COMPARATIVE STUDY OF THE TRANSCRESTAL SINUS LIFT VERSUS LATERAL APPROACH SINUS AUGMENTATION AND SIMULTANEOUS INSERTION OF BIOACTIVE CALCIUM–PHOSPHATE COATED DENTAL IMPLANTS: 7 YEARS OF FOLLOW-UP
Objectives: This prospective follow-up study aimed to compare the cumulative survival and success rate of implants with bioactive calcium-phosphate coating 7 years after insertion via lateral sinus lift with a transcrestal technique. It also aimed to evaluate bone remodelling around the elevated sinus floor. Methods: Ninety conical self-drilling implants with a calcium phosphate coating (Bioactive) were placed with a simultaneous sinus lift procedure in 40 consecutive male patients between January and December 2008 presenting with 5–6mm of residual sub-sinus bone. Their mean age at the time of surgery was 41 years. Group A (n = 20) were treated with a lateral sinus lifting procedure and simultaneous insertion of 50 implants; the graft was a mixture of platelet-rich fibrin (PRF) and deproteinised bovine bone particles (Bio-Oss) with a collagen membrane (Bio-Gide). In group B, 40 implants were inserted via a transcrestal sinus lift procedure without grafts. The time between implant placement and loading was four months. All restorations were cemented. Primary outcomes were implant survival and success rate, and secondary outcomes were modified Loe and Silness gingival index, Mombelli’s plaque index, and Mühlemann’s bleeding score. The following analyses were used to establish the dates for follow-up: implant primary and secondary stability (using resonance frequency analysis and PeriotestTM) and radiological bone changes around the implants and sinus floor. Results: All patients were seen at 4 and 12 months and followed up at 2–7 years . ISQ dates were collected during implant insertion and after 4 months of healing. The PeriotestTM dates were obtained immediately (4 months, 12 months, 7 years). After healing, ISQ values in group A were 63.1 compared with 59.1 after surgery. In group B, mean ISQ at insertion was 68.8 and 72.1 after 4 months. Mean post-surgical Periotest tm values were –2.15 for group A and −3.64 for group B. After 4 months the value for group A was −4.32 versus −4.74 for group B. The mean Periotest value for both groups after one year was −4.75 and –4.2 after 7 years. Four months after surgery, mean bone loss was –0.52mm in transcrestal cases. After one year, a bone gain of +0.16mm was observed, which decreased to –1. 3mm after 7 years. There was more bone formation after 4 months of surgery (+0.46mm) for the implants in augmented sinuses. After one year, bone loss was –0.4mm; after 7 years it was –2.1mm. The mean gain of bone height in the sinus area in group A was greater (7.8mm) than in group B (3.2mm) after surgery. After rehabilitation, group A had a gain in bone height of 7.6mm, with 7.7mm at 1 year decreasing to 2.3mm at 7 years. For group B the values were 2.9mm at 4 months, 3.1 mm at 1 year, and 3.6mm at 7 years. After 7 years, most cases (75.9%) had normal gingiva. Most implants (93%) had no plaque accumulation, and bleeding could not be provoked in 90%. There were no painful symptoms or mobility in any of the implants. Conclusion: Compared with studies on aftercare for other implant systems, the bioactive calcium–phosphate coated implant system in this study has a promising seven-year survival and success rate. This applies to partially atrophied posterior maxilla edentulous jaws and should be interpreted with respect to the patient selection criteria – transcrestal sinus lift versus lateral approach sinus augmentation with simultaneous implant insertion. The results demonstrate that Bio-Oss is a useful scaffold for augmentation in lateral approach sinus lifts. Transcrestal osteotomy and elevation of the sinus membrane with autogenous local bone is stable, and has an osteoconductive property that allows for direct contact of the implant body with newly formed bone. The resorptive processes in both techniques proceed slowly, providing sufficient time for bone maturation. -

Pectin nanocoating of titanium implant surfaces - an experimental study in rabbits
Objectives: The aim of the study was to evaluate the effect of nanocoating titanium implants with plant cell wall-derived rhamnogalacturonan-I, on bone healing and osseointegration. A new strategy to improve osseointegration and bone healing is biochemical stimulation by surface nanocoatings that may increase adhesion of bone proteins, and bone cells at the implant surface. Nanocoating with pectins, plant cell wall-derived polysaccharides, is frequently done using rhamnogalacturonan-I (RG-I). Methods: Machined titanium implants were coated with three modifications of rhamnogalacturonan-I (RG-I). Chemical and physical surface properties were examined before insertion of nanocoated implants (n = 96) into the left and right tibia of rabbits. Machined titanium implants without RG-I nanocoating were used as controls (n = 32). Total number of 128 implants was placed in tibias of 16 rabbits. Fluorochrome bone labels, calcein green and alizarin red S were given intravenously after 9 and 12 days, respectively. The bone response to the nanocoated implants was analyzed qualitatively and quantitatively after 2, 4, 6, and 8 weeks of healing using light microscopy and histomorphometric methods. Results: The RG-I coating influenced the surface chemical composition; wettability and roughness, making the surface more hydrophilic without any major effect on surface micro roughness compared to control implant surfaces.The different modifications of pectin RG-I did not significantly enhance bone healing and osseointegration analyzed after 2, 4, 6, and 8 weeks of healing compared to control implants. Although the qualitative analyses of the fluorochromes indicated a higher activity of bone formation in the mineralization front at the early stage, after 9 and 12 days at the RG-I nanocoated implants compared to the control implants although no significant quantitative difference was demonstrated. Conclusion: The present study showed that nanocoating of titanium implants with pectin RG-Is did not significantly enhance bone healing and osseointegration when placed in rabbit tibia bone. -

RELIGIOUS AND ETHICAL ATTITUDES TO USE OF ALLOGENOUS, XENOGENOUS AND SYNTHETIC TISSUE REPLACEMENT MATERIALS
Objectives: In the field of oral soft and hard tissue reconstruction, there are many data on the use and success of foreign materials of animal, mineral and synthetic origin. Religious and ethical acceptability of these materials is important in our globalised, multicultural world. The aim of our study was to determine the acceptance of allogenic or xenogenic materials among different religious groups and different polytheistics. Methods: Detailed questionnaires were handed out to twelve national leaders of various religious groups: Roman Catholic, Protestant Christian, Muslim, Greek Orthodox, New Apostolic, Romanian Orthodox, Buddhist, Serbian Orthodox, Jewish, Jehova’s Witness and Hindu. The task was to distinguish three groups according[?] to acceptance of different materials by their communities: contraindicated for ethical/religious reasons (group V); informed consent required (group C); and acceptance (group A). At the same time, 120 dentists working in oral surgeries were asked about their awareness of and publicity of ten common materials and their origins, as well as patient-information practices, and patient reactions. Results: All twelve religious groups responded to the questionnaire, mostly after seeking a qualified opinion from an international religious centre. The majority (n = 9) claimed to provide basic information for patients before undergoing any intervention. Some (n = 5) prohibited the use of animal or human tissues for religious or ethical reasons. Others (n = 2) excluded them because of the risk of disease transmission or cruelty to animals. Of the 120 polled dentists or surgeons, the minority (n = 12) were unaware of the origins of the ten described products. For a very small number of patients, the use of tissue replacement materials and the nature of the donor or origin have been important issues, but most did not approve of the use of allogeneic or xenogeneic tissue substitutes in their interventions. Conclusion:Religious attitudes to the preparation and performance of routine dental surgeries showed significant differences. From the findings, it is obvious that patients’ ethical and religious acceptance of biomaterials in this field cannot be assumed. The origin of materials should be clarified and reasonable alternatives pointed out before any intervention to prevent intercultural misunderstanding and judicial consequences.

Take this survey to help us improve your experience
on Dental Campus
For completion, you get 3 days unlimited access to:
- All lectures
- All cases
- All videos