








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


Patient-Reported Outcome Measures
based on the book chapter by Colman McGrath Summary There has been a surge of interest in patient-reported outcome measures (PROMs) in all areas of clinical research. Assessing the patients own perceptions of their health, quality of life, functional ability and experience of pain provides very valuable information on the success of an intervention. This chapter describes the development of some commonly used instruments, and summarizes their limitations and suitability for different studies in implant surgery and tissue regeneration. It advises investigators on the selection of different types generic, condition-specific, dimension-specific and utility measures. The authors explain why general (global) instruments like the popular Short Form SF-36 questionnaire have limited sensitivity for oral outcomes, suggesting several condition-specific tools that yield far more specific data and are quick to complete, making them suitable for studies in busy clinic settings and large numbers of patients. The authors describe the role of health utility indexes, which allow patients to rank the importance of items affecting their quality of life, or permit costbenefit analysis of an intervention. The instruments are discussed in the context of their appropriateness for a particular study, their acceptability to patients, validity, reliability and reproducibility, and their responsiveness to change. In terms of interpretation, emphasis is placed on the challenge of identifying the minimally clinically important difference (MCID). Open full-text PDF (0.9 MB) -
Endpoints In Oral And Maxillofacial Regeneration Clinical Trials
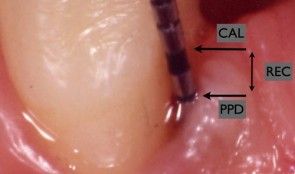
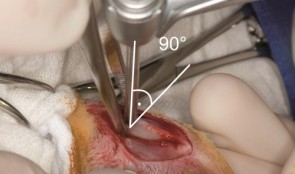
based on the book chapter by Mariano Sanz and Fabio Vignoletti Summary Selection of endpoints, or outcome measures, can be daunting for researchers because of the huge variation in disease processes and outcomes relating to implants, surgery and tissue regeneration, and factors such as the research question and study design. This chapter advises investigators on the selection of valid, patient-applicable, sensitive, specific, ethical endpoints, that do not damage tissue integrity. It defines the terms, and distinguishes between true and surrogate and primary and secondary endpoints. It explains about different types biological, clinical, psychological and economic -- and summarizes their limitations and value, such as biological measures for disease etiology and progress, and clinical measures for assessing survival and function. The authors focus on common parameters relating to periodontal probing, bone radiography and patient-related outcomes, and describe the relevance of numerous specific endpoints in studies of localized gingival recession, soft tissue augmentation and mandibular furcation regeneration. They also review endpoint selection in implant therapy, for evaluating bone regenerative therapies, protocols for socket preservation and immediate implantation, lateral and vertical bone augmentation, and implant-supported restorations. Throughout the chapter, the chosen endpoints are related to the wider aspects of patient selection, randomization and compliance, data collection and observer variation, error proneness and reporting of results. Open full-text PDF (2.3 MB) -

Vertical Ridge Augmentation
Vertical augmentation is essential for restoring bone defects in patients with destructive gum disease, before rigid fixation of implants or grafts. However, in practice it is associated with high complication rates and limited success. Thus it is important to refine the techniques used by dental surgeons through preclinical research. This chapter looks at various animal studies, and focuses on one specific validated, reproducible and reliable protocol. This involves creating a saddle-like, bony, critical-size defect in the mandible of dogs, in which sufficient time is allowed for the defect to become chronic, thus mimicking bone atrophy in humans. Vertical bone gain is assessed following placement of a tissue-engineered block. Surgical and flap management techniques can be tested, as well as different biologics, devices, scaffolds, membranes, implants and screws. Assessment relates to the initial defect, as well as responses over time relating to resorption of graft particles, soft tissue swelling and inflammation and bone destruction and formation. Osseointegration is quantified to indicate success or failure of the intervention. The protocol can also be used to compare analytical methods. The methods have fairly predictable outcomes, and are applicable to patients with traumatic tooth extraction, jaw damage, endodontic infections and failed implants. -

Sinus Floor Augmentation
The maxillary sinuses are located inside the cheekbones, above the upper jaw, from the second premolar area to the wisdom teeth. In some people with tooth loss, the sinuses are too close to the upper jaw for dental implants to be placed; in others, bone may have been reabsorbed because of gum disease. In either case, bone height can be restored using a sinus lift – an increasingly common technique in dental practice. A small hole is made in the bone beneath the gum and the membrane lining the sinus is pushed away from the jaw to create a space into which bone graft material can be packed. Implants can then be placed after the graft has integrated with the natural tissue. Preclinical models are necessary for testing bone grafts from different sources, and different bone substitution materials, biologically active coatings, growth factors, and implant types. The vascularization process can also be investigated. This chapter discusses the merits of various animals for studying the pathology and repair of sinus defects, with a preference for those with similar sinus structures, bone loading characteristics and remodeling processes to humans. Osseointegration of graft materials can take many months, so the protocols here provide a framework of suitable timings and sequences of surgical procedures, including the placing of implants at same time as augmentation. Suitable endpoints are defined too to assist investigators in planning and reporting on reproducible, relevant outcomes. -

Peri-implantitis Defect
Inserting implants immediately after tooth extraction reduces clinic appointments, but some patients experience breakdown of their gum and bone tissues; this early exposure of the implant inhibits bone regeneration and implant success. Increasing numbers of people have implants nowadays, more of which contain titanium, which is good for osseointegration, but tends to harbor bacteria if the surrounding bone shrinks away. Preclinical research is therefore important for investigating the nature of implantitis and its relations to bacterial plaque formation. Flap procedures need to be optimized to ensure adequate wound closure and prevent wound breakdown. To this end, inflammation resembling that encountered by dentists is induced in animals by allowing plaque to accumulate or placing cotton ligatures on the gum. It is difficult to create standardized defects, but valuable observations can be made on the timings of extraction and implantation, healing periods and plaque control. The efficacy of treatments for preventing tissue loss can be assessed, as well as options for antimicrobial decontamination. Investigators can rely on the clinical relevance of the endpoints described here, which involve assessment by probing of peri-implant pockets, determining the level of the alveolar bone crest, the amount of bone–implant contact and the extent of inflammatory cell infiltrates. This remains a rich area for research in a growing area of practice. -
Compromised Bone Healing
The bone healing process in people can be affected by diseases such as Crohn’s disease, diabetes and colitis. It can also be affected by drugs such as bisphosphonates, which are used to treat weak bones in people with osteoporosis, Paget's disease and certain cancers. The role of animal models is enormous for investigating these disease conditions as well as other “risk factors” for compromised healing, such as radiotherapy, which is being increasingly used as early treatment of cancer in the community rises. Diabetes and intestinal disorders can be induced in rats, often using chemicals with toxic effects, but the diseases can take some time to develop. This chapter gives guidance on various timeframes for evaluating inflammatory processes, osseointegration and collagen cross-linking, and gives details on mechanical strength testing of dental implants and other candidate therapies. Different aspects of the compromised bone healing response can be observed using both the long bones (tibia and femur) and the maxilla of rats. This chapter also describes an adaptable study protocol for new investigators, with suitable endpoints such as bone to tissue ratio and bone to implant contact, to contribute to the body of knowledge on patients with compromised bone healing who are increasingly encountered in dental practice. -

Regulatory And Good Clinical Practice Aspects In Clinical Practice
based on the book chapter by Gudrun Denke Summary It is critical for researchers conducting patient-oriented research to attend to the regulatory aspects of their studies and employ good clinical practice (GCP) throughout. This chapter provides an overview of GCP in both Europe and the USA, with valuable summaries of the many processes involved when preparing to conduct trials on medical devices, drugs and biologics in regenerative surgery, with a particular focus on the content and scope of ISO 14155:2011. The regulatory documentation is described, such as investigator brochures, case report forms, and clinical investigation plans. They authors go into detail about meeting ethical, quality and national standards through appropriate clinical investigation planning and monitoring. They draw attention to the roles and functions of sponsors and principal investigators, as well as CE marking and trial termination. The importance of assigning risk to medical devices and products is also discussed, whereby absorbable materials, bone morphogenic proteins, dental lasers and subperiosteal implants are deemed to carry significant risks, while caries-removal solutions, fillers and traditional cushions pads are considered insignificant. The four phases of trials for drugs and biologics are also outlined, together with the need for a separate classification scheme for medical devices that comprises exploratory (first-in-human), confirmatory (safety and efficacy) and post-marketing follow-up (improvement) phases. Open full-text PDF (1.1 MB) -
Ethical Aspects In Clinical Research
based on the book chapter by Klaus Peter Rippe Summary This chapter deals with the moral and ethical minefield faced by all investigators conducting clinical experiments in patients. Obtaining histological material for studies of tissue regeneration can be ethically compromising, and any intervention may lead to burdens as well as benefits for patients, even after robust studies in animal models. In the absence of a clear concensus on morality or a simple philosophical stance, the authors focus on the principals of proportionality and equipoise, the potential for risk, international justice, and protecting patients from exploitation due to geographical or socioeconomic factors. They stress the importance of obtaining voluntarily consent from every participant, or surrogate decisions for vulnerable patients, and highlight the need for leaving no doubt about what might happen during the trial and the potential for harm. The obligation to help all patients poses unique issues: some are simply fixed, for example by comparing a new therapy with the current best one (rather than no therapy or placebo); and others are complex. However, it is acknowledged that when a particular trial arm offers more potential than one or more other arms of the study, any patient who gains a benefit also provides a means to benefit others. The doctorpatient relationship is also examined in this chapter, particularly clinicians who must recruit their own trial participants, for example when conducting preventive oral health trials among school-children. Open full-text PDF (1 MB) -

Development Of A Clinical Research Protocol
based on the book chapter by Maurizio S. Tonetti Summary Clinical investigations that fail to provide clear and relevant answers are a waste of valuable resources. This chapter describes how to avoid common pitfalls at the proposal stage, such as rejection by an ethics committee, or producing meaningless study results. With reference to ISO-14155-2011 throughout, the authors offer guidance on writing robust clinical protocols, formulating clinically relevant questions, and designing experiments that align directly with the clinical question. In the context of equipoise and ethical soundness, the practical aspects of patient selection, bias, sample size, trial arms and control groups, are addressed, as well as blinding and randomization, data collection and analysis, and obtaining meaningful outcome measures. Among these are patient-related outcomes (PROMs), which are increasingly important for identifying therapies that produce relatively less discomfort and better esthetics. When it comes to protocol design, prevention rather than cure is clearly preferable; among the issues raised are identifying potential errors and taking corrective action at the protocol stage; collaborating with all stakeholders including statisticians and administrators during the development stage; using the peer review process to improve chances of ethical approval; and allowing public and academic access to the protocol via trial registries, in order to aid recruitment, enhance collaboration, identify gaps in the research, and prevent duplication of studies. Open full-text PDF (1.1 MB) -

Management Of A Clinical Study
based on the book chapter by Jeanie Suvan Summary The focus of this chapter is on the appointment of a study manager to maximize the success of a clinical investigation. It explains the role of study managers (as distinct from principal investigators) in clinical trials, from initiation to study closure, applying project management principles from chairside to site facility. They use tailored planning strategies and tools including checklists, agendas, schedules, databases and spreadsheets, to deal with administrative and financial matters, standard operating procedures, timelines, logistics and auditing. Their involvement begins with translation of the protocol into reality and meeting regulatory requirements, through to data collection, adverse event recording and collation of documents in site files. The authors point out how good study managers identify limiting factors and barriers, prevent serious errors from occurring, and ensure all phases of the study flow smoothly. Their invaluable contributions include budgeting and tracking systems, devising formulae for calculating resources and clinic time, and contingency plans for coping with equipment failures and sickness absence. They contribute to team training, motivation and communication, and collaborate externally with ethics committee, funders, sponsors and report writers. They also help with patient recruitment, gaining informed consent, monitoring and retaining patients, and ensuring compliance. This information provides a compelling case for engaging a study manager. Open full-text PDF (1.1 MB)