








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


Intraorally Fabricated, Glass Fiber Reinforced Composite Bridge for Replacement of Individual Anterior Teeth - The entire case
Hugo, BurkardProcedure: - Introduction and establishment of indication for the treatment - Bridge construction with glass fiber reinforcement - Presentation of the patient with congenital absence of teeth # 12 and 22 - Clinical procedure for fabrication of a bridge for tooth #22 - Discussion of the technique Contents: Here, we describe a technique for direct application of composite bridges with adhesive bonding. The procedure is designed to provide a replacement for individual anterior teeth, especially in younger individuals who have lost a tooth due to trauma or who have congenitally missing teeth. Bridge manufacture is completely intraoral. By using a one or two-wing abutment design, a framework of parallel, pre-impregnated glass fibers is adhesively bonded, and the midsection is freely built up from composite by a special procedure. This systematic approach permits reasonably priced manufacture of direct tooth replacements with predictably good esthetic results. Maximal conservation of substance and reversibility, which is achieved by dispensing with prepping measures, means that the procedure does not limit the possibilities for future restorations (e.g., implants). -

Regenerative Measures for Osseous Defect Repair and Optimal Esthetics
Sculean, AntonProcedure: Theoretical Part: - Adult male with a deep and broad intraosseous bone defect located on tooth #13 - The indication for modified papilla preservation in the scope of regenerative therapy was established based on the width of the diastema - Regenerative periodontal therapy with Emdogain and a Bio-Oss® cancellous bone graft - Emdogain is applied to the root surface to stimulate regeneration of periodontal structures - To prevent graft collapse and to minimize the risk of development of too large a recession in this esthetically important region, the defect was filled with Bio-Oss® cancellous bone material Practical Part: - The papilla preservation technique was performed using microsurgical instruments - The root surface area was conditioned with 24% EDTA for ca. 2 minutes - Emdogain was applied to the root surface - The defect was filled with the Emdogain/Bio-Oss® mixture - The wound was closed with two mattress sutures one horizontal mattress suture to secure the graft in place, and a second modified vertical mattress suture to tightly close the papilla - A 5-0 suture was used for the horizontal mattress suture, and a 6-0 monofilament was used for the vertical mattress suture - Postoperative care entailed rinsing the wound twice daily for 4 weeks with 0.2% chlorhexidine and ibuprofen analgesia on the first few days after surgery Contents: The patient's jaw displayed a generalized loss of clinical attachment and alveolar bone. His general history was unremarkable; the patient was a non-smoker. Microbiological tests showed large numbers of Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis. The diagnosis was "generalized aggressive periodontitis". After four months of initial therapy consisting of antibiotic combination therapy (amoxicillin + metronidazole), intraoral radiographs showed a deep and wide intraosseous bone defect located mesial and palatal to tooth #13. To preserve this strategically important tooth we opted to perform regenerative therapy with Emdogain and Bio-Oss cancellous bone material. Ten months after regenerative periodontal therapy, the probing depth had decreased by 7 mm, and 5-6 mm of clinical attachment had been gained. At this time, the probing depth was 2-3 mm and intraoral radiographs showed near-complete filling of the osseous defect. -
Regenerative Procedures for Optimized Esthetics at Tooth 11
Schlee, MarkusContents: - Exploration - Incision and Flap Mobilization - Palatal Flap Preservation with Interdental Tissue Preservation - Detoxification and Concrement Removal at 11 - Harvesting of Autogenous Bone Chips from the Spina Nasalis - Conditioning of the Root Surface with EDTA-Gel - Application of Emdogain and Filling of the Bone Defect - Wound Closure Synopsis After Finishing the Initial Treatment for Aggressive Periodontitis, Regenerative Treatment of a Tunnel-Shaped Pocket at Tooth 11 was attempted. Rotation and Crowding of the Buccally Inclined Tooth represented a favorable Etiological Factor. The patient did not wish to receive Orthodontic Treatment to eliminate this Causal Factor after Completion of Primary Treatment. Treatment was therefore limited to the Surgical Regeneration Attempt. The Interdental Space was larger than 3 mm and the Bone Pocket was a mostly Three-Walled Structure, so the Chances of Success were considered to be good. Exploration was first performed to identify the Course of the Defect Margins. Exact knowledge of the Bone Anatomy in all three Planes is essential to successful Incision Planning. A Tunnel-Shaped Defect delimited by Bone in the Region of Tooth 11 with good chances of Periodontal Regeneration was found. A major Challenge of this Procedure is the need to keep the Defect completely covered with Soft Tissue throughout the Healing Process. Cortellini's Papilla Preservation Technique was used for this Purpose. After Incision and Flap Mobilization, it became evident that the Defect only had two Walls in the Coronal Region and that Bone was lacking in the Buccal Region. According to the current Data on Periodontal Regeneration, the Attachment Gain achieved using an Enamel Matrix Protein (Emdogain®) alone can be just as good as that achieved using Emdogain and Bone Graft Material combined. Still, we elected to use a Combination Technique in the Present Case because it provides better Papillary Support. The Graft Material consisted of Autogenous Bone Chips from the Spina Nasalis, which can easily be harvested by Means of the Piezo Technique After gentle Detoxification, the Root Surface was treated with Emdogain. The Defect was then filled with Autogenous Bone Chips and closed by Microsurgical Suture Techniques. Six months after Surgery, Partial Regeneration of the Papilla can be seen. -

Mandibular Distraction Osteotomy
Schleier, Peter / Schultze-Mosgau, StefanProcedure - Indications and preoperative planning - Incision technique and osteotomy - Placement of distraction apparatus - Wound closure and postoperative regimen Materials: V2-Alveolar distractor, Medartis (Switzerland) 2,0mm Screws for Osteosynthesis, Medartis (Switzerland) Vicryl Suture, Ethilon (USA) -

Regenerative Treatment on Tooth 14 und 24
Eickholz, PeterProcedure: - Incision - Flap Design - Removal of the granulation tissue - Application of the PrefGel on the root surface - Application of the Enamel -Matrix -Protein (Emdogain) - Suture (Offset-Suture) - Identical procedure on the opposite side (1st quadrant) Materials: Retractor Micro Surgical Scalpel Handle Mini Scalpel Blades 4 x Gracey Curettes Periosteal Trombelli Periosteal Prichard Microsurgical Needle Holder Castroviejo Scissors Tweezers Microsurgical Tweezers Gore Tex CV-5 Sutures Gore Tex CV-6 Sutures Emdogain 0,7 ml PrefGel -

-

Surgical Techniques for Closure of Oro-Antral Communications
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: With a maxillary sinus recess reaching far into the alveolar process of the maxilla, the maxillary sinus can sometimes be opened when maxillary incisors are extracted. An oro-antral communication is determined by a nose-blowing test or by sounding out of the alveolus with blunt probes. After an inflamed, cystic, or tumorous maxillary sinus illness has been excluded, an oro-antral communication should be closed immediately with plastic surgery within the first 24 hours after extraction to prevent the germ-free maxillary sinus from being contaminated. Plastic covering by plastic surgery using a cheek flap with vestibular stem is demonstrated. After a mucoperiosteal flap with vestibular stem has been formed, the flap is lengthened by slitting the periosteum so that a tension-free sealing of the opened maxillary sinus will be possible without endangering the flap's blood flow at the same time. Outline: - Diagnostics of an oro-antral communication - Exclusion of inflammatory, cystic, or tumorous maxillary sinus illnesses - Cheek flap plastic surgery for plastic covering of an oro-antral communication: - Cutting direction for the formation of a mucoperiosteal flap with vestibular stem; - De-epithelalization of wound margins; - Mobilization of the flap by slitting the periosteum; - Periosteal holding stitches for tension; - free closure of the oro-antral communication; - Stitching technique for saliva-proof wound closure. - Demonstration of buccal flap plastic surgery - Demonstration of bridge flap plastic surgery - Demonstration of palatal flap plastic surgery - Postoperative reaction measures -
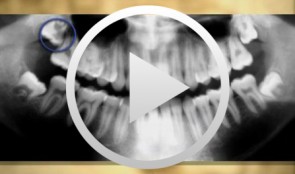
Operative Therapy for Retained Teeth in the Maxilla
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: In adolescence, the exposure and orthodontic classification of retained teeth, especially canines and premolars, represents a useful therapy measure. Techniques for surgically exposing vestibularly and palatally retained teeth are demonstrated using the tubed pedicle flap technique. Because epithelialized mucous membrane is covered in the tubed pedicle flap technique, a renewed growth of the exposed tooth is prevented and a classification of the tooth with orthodontic appliances under sight control is enabled. Depending on the retention form, the extent of movement, and the patient's age, exposure may no longer be possible under some circumstances, indicating the need for operative removal of the retained canine or premolar. Preoperative localization methods, vestibular and palatal operative access paths, and surgical techniques for atraumatic removal are demonstrated. Operative techniques for the atraumatic removal of retained maxillary third molars also are shown. For the gentle removal of retained maxillary third molars, it is very important to record their topographic positional relationship to the maxillary sinus and to select the cutting direction and most suitable osteotomy technique. Outline: - Techniques for exposing maxillary canines or premolars for orthodontic classification - Operative removal of retained maxillary canines - Operative removal of retained maxillary third molars -

Sinus Floor Augmentation with Autogenous Chin Bone Grafts
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: In the maxillary incisor region, a sinus floor augmentation to enlarge the vertical bone supply may be indicated for a vertically reduced local bone height of less than 5 to 7 mm before procedures to rehabilitate masticatory function with an implant-bearing tooth replacement. For a single-sided deposit osteoplasty, the quantity of autogenous bone from the chin region is usually sufficient. The operative procedure of a single-sided lateral sinus floor augmentation is demonstrated with particulate spongious bone and alternatively with an autogenous block graft. The video also shows the operative method for a crestal sinus floor augmentation with the aid of the endoscopically controlled condensation technique. The advantages and disadvantages of the individual procedures are highlighted. In addition, the technique for harvesting chin bone transplants in different case examples is shown. Outline: - Operative technique for lateral sinus floor augmentation with autogenous particulate spongious bone - Operative technique for lateral sinus floor augmentation with autogenous block grafts - Crestal, endoscopically controlled sinus floor augmentation with condensation technique - Techniques for harvesting chin bone grafts - Range of indication for sinus floor augmentation - Lateral sinus floor augmentation - Operative technique of crestal, endoscopically controlled sinus floor augmentation - Operative technique of autogenous chin bone removal -

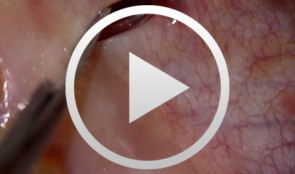
Defect Prevention following Extraction of a Maxillary Central Incisor
Zuhr, OttoContents: - Minimally invasive, atraumatic extraction of an anterior tooth - Buccal soft tissue augmentation using a modified tunneling technique - Socket preservation technique for conservation of the extraction socket - Provisional restoration and closure using modified suspension sutures Materials Checklist: Tunneling Knife® (Dr. Zuhr), No. 1 / No. 2 Keydent Microblade SR Geistlich Bio-Oss® Spongiosa, particle size 0.25 - 1 mm Geistlich Bio-Gide® membrane, 25 x 25 mm Seralene Blue 7/0 DS-15, 0.5 m sutures CV-5 Gore-Tex sutures