








-
- English
- Deutsch
- Spanish
-
- General Diagnostics
- Treatment
- Tools/Materials
- Basic/General Knowledge
- Research
- Events
- Organisations
-
-
-
-
-
-

-


-
Operative Therapy for Retained Teeth in the Maxilla
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: In adolescence, the exposure and orthodontic classification of retained teeth, especially canines and premolars, represents a useful therapy measure. Techniques for surgically exposing vestibularly and palatally retained teeth are demonstrated using the tubed pedicle flap technique. Because epithelialized mucous membrane is covered in the tubed pedicle flap technique, a renewed growth of the exposed tooth is prevented and a classification of the tooth with orthodontic appliances under sight control is enabled. Depending on the retention form, the extent of movement, and the patient's age, exposure may no longer be possible under some circumstances, indicating the need for operative removal of the retained canine or premolar. Preoperative localization methods, vestibular and palatal operative access paths, and surgical techniques for atraumatic removal are demonstrated. Operative techniques for the atraumatic removal of retained maxillary third molars also are shown. For the gentle removal of retained maxillary third molars, it is very important to record their topographic positional relationship to the maxillary sinus and to select the cutting direction and most suitable osteotomy technique. Outline: - Techniques for exposing maxillary canines or premolars for orthodontic classification - Operative removal of retained maxillary canines - Operative removal of retained maxillary third molars -

Regenerative Treatment on Tooth 14 und 24
Eickholz, PeterProcedure: - Incision - Flap Design - Removal of the granulation tissue - Application of the PrefGel on the root surface - Application of the Enamel -Matrix -Protein (Emdogain) - Suture (Offset-Suture) - Identical procedure on the opposite side (1st quadrant) Materials: Retractor Micro Surgical Scalpel Handle Mini Scalpel Blades 4 x Gracey Curettes Periosteal Trombelli Periosteal Prichard Microsurgical Needle Holder Castroviejo Scissors Tweezers Microsurgical Tweezers Gore Tex CV-5 Sutures Gore Tex CV-6 Sutures Emdogain 0,7 ml PrefGel -
Mandibular Distraction Osteotomy
Schleier, Peter / Schultze-Mosgau, StefanProcedure - Indications and preoperative planning - Incision technique and osteotomy - Placement of distraction apparatus - Wound closure and postoperative regimen Materials: V2-Alveolar distractor, Medartis (Switzerland) 2,0mm Screws for Osteosynthesis, Medartis (Switzerland) Vicryl Suture, Ethilon (USA) -

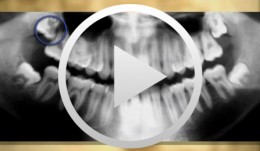
Treatment Concept for Extracting Impacted Lower Wisdom Teeth
Schultze-Mosgau, Stefan / Neukam, Friedrich Wilhelm / Basting, GerdContent: The removal of retained mandibular third molars is one of the most commonly performed surgical procedures. Because of the close anatomic positional relationship of the third molars to the adjacent teeth and to the inferior alveolar nerve, there is a risk of damage to the surrounding structures during surgical removal. For uncomplicated removal, knowledge of the different retention forms and a suitable atraumatic operation technique is important. After the block anesthesia of the inferior alveolar nerve and the buccal nerve, the cutting direction must be determined so that a mucoperiosteal flap with vestibular stem can be lifted. After the lingual subperiosteal insertion of a rasp to protect the lingual nerve, the third molar is exposed by buccal osteotomy with ball-shaped hard metal burs as far as its largest circumference and removed by careful luxation movements. Outline: - Schematic and radiologic demonstration of the different retention forms of low retained third molars and illustration of the indications for removal - Preparation of treatment documents and an explanatory discussion showing potential complications - demonstration of the surgical procedure: local anesthesia, cutting direction, protection of the lingual nerve, osteotomy, stitching technique -

Bone Spreading, Bone Condensing (Split Control System)
Streckbein, Roland -

Bone Transplantation with Systemized Armamentarium
Streckbein, Roland -

Gap Closure with a Minor Incisal Edge Restauration
Klaiber, BerndProcedure: - Incisal edge restoration at Tooth 11 - Sketch prior to widening procedure in anterior teeth region - Placement and shaping of matrix band retainer used for tooth widening - Application of composite material and spreading with small Heidemann spatula to establish stable and broad approximal contact - Application of dentin and enamel composite - Shaping and completing; positioning of the lateral edge lines; shaping the interincisal triangle. - Creation of an invisible transition, composite/enamel, with scalpel #15 - Polishing Materials Adhesive: Optibond Fl (Kerr) Composite: Enamel HFO (Micerium) Dentin UD4, UD3,5 and UD3 Enamel GE2 Opalescence OBN Flowable Composite: Tetric Flow A4 (Vivadent) Temporary Composite for shaping of matrix band retainer SystepOnlay (Vivadent) -

Regenerative Treatment of Class II Mandibular Furcation Defects
Heinz, BerndProcedure Case description: -Class II furcation defect at teeth 46 and 47 and gingival recessions at teeth 43 and 44 - Root planing using PerioSet - Incision technique - Cleaning furcation defect at tooth 46 - Pref Gel application, rinsing and Emdogain application - Insertion of Bio-Oss into the furcation space with an amalgam plugger after hydration - Condensation of the bone replacement material and application of an absorbable membrane (Bio-Gide) - Atraumatic suture closure using 6/0 Seralene Contents: This video demonstration shows the simultaneous treatment of recessions at teeth 43 and 44 and of class II furcation defects at teeth 46 and 47. After a brief case description, root planning is done using PerioSet. Next, an incision is made and the furcation defects are very carefully cleaned using hand instruments and ultrasonic scalers (Soniflex). The cleaned root surfaces and furcation defects are conditioned with Pref Gel (Straumann) for two minutes. The objective of conditioning is to remove the smear layer, to open the dentine tubules, and to enable surface demineralization. Moreover, this measure serves to optimize the contact between Emdogain and the root surface. After two minutes, the EDTA suspension is removed using physiological saline solution or water spray. Immediately afterwards, Emdogain is applied to the blood and saliva-free root surface. This procedure was also used to treat the furcation defect at tooth 47. Regenerative treatment of tooth 46 was performed since that tooth had a very extensive furcation defect. The defect was filled with Bio-Oss, which was applied using an amalgam plugger. Absorbable Bio-Gide was used for coverage of the furcation entrance. Finally, the wound was closed using loop sutures and single interrupted sutures. -

Flap designs for Interdental Tissue Preservation in Periodontal Therapy
Salvi, Giovanni E.Procedure: - Introduction: History -Taking, Examination, Diagnosis, Etiology, Prognosis for Individual Teeth - Four - Phase Treatment Sequence - Modified Papilla Preservation Technique(MPPT) - Simplified Papilla Preservation Technique (SPPT) - Findings 6 months after Surgery Synopsis The Modified and Simplified Papilla Preservation Techniques for conservation of interproximal papillary tissue were designed to provide access to deep and narrow bony defects to enable regenerative periodontal treatment. The Modified Papilla Preservation Technique (MPPT) was designed to ensure tension-free primary closure via barrier membranes in patients with small interdental spaces. The Simplified Papilla Preservation Technique(SPPT) is used to gain access to narrow interdental spaces ( < 2mm) and to deep defects in the lateral tooth region. Apart from preserving primary wound closure in the interdental space, the two techniques also serve to keep the membrane from collapsing into the bony defect. Both MPPT and SPPT employ special suture techniques to ensure tension-free primary closure of the interdental space. This video clip also serves to demonstrate that the two techniques of interproximal tissue preservation can also be used for periodontal interventions without regenerative measures. -

Regenerative Measures for Osseous Defect Repair and Optimal Esthetics
Sculean, AntonProcedure: Theoretical Part: - Adult male with a deep and broad intraosseous bone defect located on tooth #13 - The indication for modified papilla preservation in the scope of regenerative therapy was established based on the width of the diastema - Regenerative periodontal therapy with Emdogain and a Bio-Oss® cancellous bone graft - Emdogain is applied to the root surface to stimulate regeneration of periodontal structures - To prevent graft collapse and to minimize the risk of development of too large a recession in this esthetically important region, the defect was filled with Bio-Oss® cancellous bone material Practical Part: - The papilla preservation technique was performed using microsurgical instruments - The root surface area was conditioned with 24% EDTA for ca. 2 minutes - Emdogain was applied to the root surface - The defect was filled with the Emdogain/Bio-Oss® mixture - The wound was closed with two mattress sutures one horizontal mattress suture to secure the graft in place, and a second modified vertical mattress suture to tightly close the papilla - A 5-0 suture was used for the horizontal mattress suture, and a 6-0 monofilament was used for the vertical mattress suture - Postoperative care entailed rinsing the wound twice daily for 4 weeks with 0.2% chlorhexidine and ibuprofen analgesia on the first few days after surgery Contents: The patient's jaw displayed a generalized loss of clinical attachment and alveolar bone. His general history was unremarkable; the patient was a non-smoker. Microbiological tests showed large numbers of Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis. The diagnosis was "generalized aggressive periodontitis". After four months of initial therapy consisting of antibiotic combination therapy (amoxicillin + metronidazole), intraoral radiographs showed a deep and wide intraosseous bone defect located mesial and palatal to tooth #13. To preserve this strategically important tooth we opted to perform regenerative therapy with Emdogain and Bio-Oss cancellous bone material. Ten months after regenerative periodontal therapy, the probing depth had decreased by 7 mm, and 5-6 mm of clinical attachment had been gained. At this time, the probing depth was 2-3 mm and intraoral radiographs showed near-complete filling of the osseous defect. -

Microsurgical Removal of a Foreign Body from the Mandibular Canal
Schultze-Mosgau, StefanOverview: - Access and incision: Creation of a vestibular pedicled mucoperiosteal flap via a gingival margin incision while preserving the papilla - Removal of vestibular bone in the region of tooth 46 using a microsurgical instrument - Exposure of the neurovascular bundle - Removal of the foreign body - Re-adaptation of the mucoperiosteal flap - Wound closure with atraumatic suture material Contents: Female patient with an indication for microsurgical foreign body removal (removal of a fractured root canal instrument from a previous endodontic treatment of tooth 46) using a surgical microscope. The foreign body extends from the apex into the mandibular canal.